
A Trusted Place for Answers about Your Back & Leg Pain
Last Updated: 12/17/25
A Trusted Place for Answers about Your Back Pain
A Trusted Place for Answers
Welcome to ChiroGeek's Spine Research Review/Blog!
On this page, Dr. Gillard reviews some of the most important spine research papers of modern times. The latest review is on top.
Last Updated: 9/24/24
Brouwer PA, et al. “Percutaneous Laser Disc Decompression versus Conventional Microdiscectomy in Sciatica: a Randomized Controlled Trial.” Spine J (impact factor 4.3); 2015; 15(5):857-65.
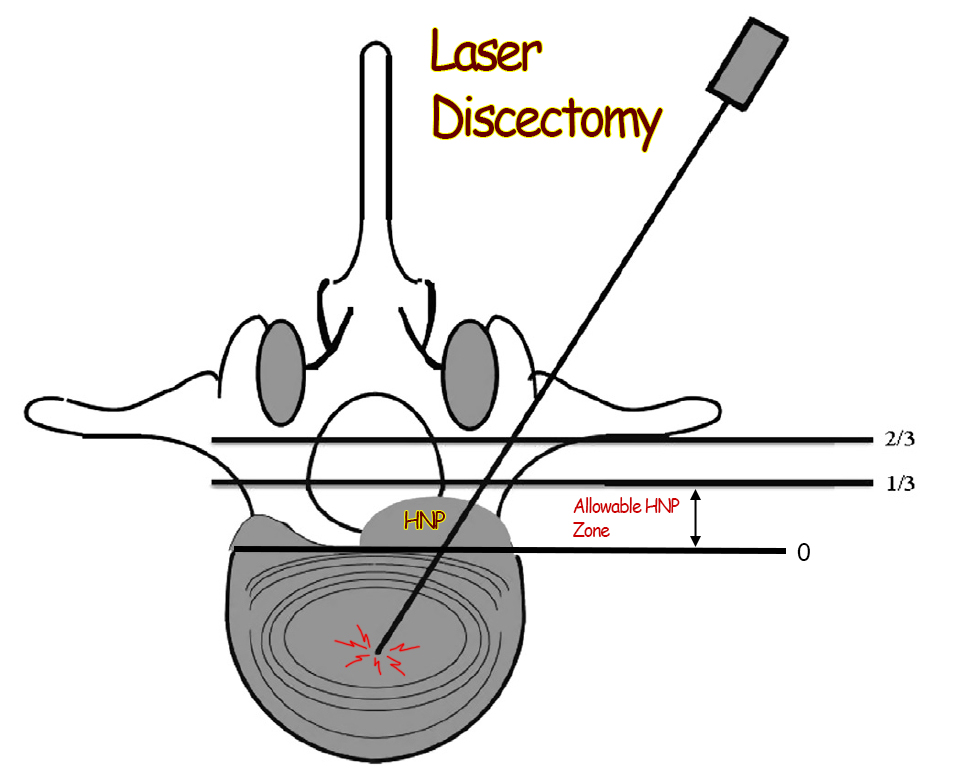
Laser Discectomy for Disc Herniation? Let’s see what the very first randomized control trial, which compared traditional open microdiscectomy to laser discectomy, has to say about this.
Did you know it took 24 years after FDA approval for a research group to finally test the effectiveness of laser discectomy by putting it up against traditional open microdiscectomy in a multiclinic randomized control trial? I was shocked to learn this, as I started digging into this treatment intervention. Let's talk about the 2015 Brouwner et al study:
In this Dutch study, Brouwer et al put laser discectomy (aka, percutaneous Laser disc decompression) against the undisputed gold standard, conventional open microdiscectomy, for the treatment of patients with disc herniation-related back and lower limb (sciatica) pain.
It’s important to note that only small disc protrusions (i.e., herniations that occupied only 1/3 or less of the anterior epidural space {see diagram}) were allowed into the study. Moderate and large sized disc herniations were excluded from the study and were treated with traditional open discectomy. Also, disc herniations that did not cause adjacent nerve root contact/compression were not allowed in the study.
STUDY DESIGN
one-hundred and fifteen (115) patients, all of whom suffered a symptomatic small lumbar disc protrusion, were randomly placed into one of two treatment groups: traditional open microdiscectomy group or a laser microdiscectomy group. Note: sometimes the Dutch use the word "decompression" in place of microdiscectomy. These surgeries took place at several different clinics and were performed by y several different physicians, which is most excellent! Therefore, we have the ultimate study going on here: a randomized controlled multi-clinic trial.
After the surgery, the patients were carefully followed for the next year and periodically reassessed with regard to their functional status and amount of pain in the low back and lower extremity. Note: a one-year follow-up is a little short. Typically, most top Spine Journals demand two years of follow-up, so I'm not sure how this study snuck in to The Spine Journal.
RESULTS:
Shocking, the laser discectomy failed in 44% of those patients enrolled, which in turn forced them into at least one reoperation within 12 months! Also surprisingly, 16% [still an unacceptably high level] of the open discectomy group failed and needed a reoperation within one year. This number is obviously statistically significant. [Statistically significant? There’s no question that the laser discectomy group had way more need for second surgery compared to the open discectomy group– it wasn't just chance that made this difference.]
Why Such High Failures? The author suggested that the high failure rate in both groups was secondary to the fact that 33% of the patients waited for more than 12 months to have the surgery. [note: it is well known that you should not wait for more than about four months, if you going to have to discectomy surgery for a symptomatic disc herniation].
Surgical Complications:
Surprisingly, there was a 11% complication rate in the open discectomy group (unusually high) compared to a 5% complication rate in the laser discectomy group.
Outcomes
With regard to functional outcomes (i.e., how the patients did with regard to being able to go back to work and/or how they could perform the usual activities of daily living), it was difficult to understand how the 44% failed laser discectomy patients were treated after the failure. It appears that their failure to respond to laser discectomy was not held against laser discectomy. They simply transferred these patients into the microdiscectomy group. If this is what happened (this was a terribly written paper! I'm guessing it was written in Dutch and somebody did a poor job of translated into English), that's not fair to say that there was no difference with regard to functional outcomes between the two groups, which is what they said.
With regard to patient-reported outcomes, as assessed by the classic visual analog scale (VAS), (VAS= ask patient: how much pain do you have on a scale of 0 to 10, where 10 is horrible in the hospital-type pain and zero is no pain), the laser discectomy group did not do well, as they had more residual leg pain at 24 months (p>0.05 = statistically significant difference), compared to the microdiscectomy group.
MY CONCLUSION:
Laser discectomy for the treatment of small symptomatic disc protrusions had a terrible performance, when it was put up against the gold standard disc herniation treatment, open microdiscectomy. Specifically, 44% of the patients in the laser discectomy group failed to respond to that treatment and had to be treated with other types of surgery [Note: the authors didn't say what the other types of surgery were]. Furthermore, laser discectomy patients suffered worse residual lower extremity pain (sciatica), compared to traditional open microdiscectomy.
This terrible performance of laser discectomy likely gave insurance companies plenty of evidence to deny benefits for laser discectomy. Why would you pay for something if 44% are going to need another surgery within 12 months?
Another huge problem with laser discectomy is the fact that there are no other randomized controlled trials for for laser discectomy! Unbelievable! I would speculate that doctors who tout this procedure are fearful of getting results like Brouwer et al got, and therefore just don't dare put their laser discectomy technique up against traditional open or endoscopic microdiscectomy technique. I seriously doubt that insurances will ever cover this procedure.
The results of this study, as well as the nonexistence of any other randomized controlled trials is the reason I do not recommend any type of Laser Disc surgery for my clients.
Final note: this was a terribly written paper and was filled with mistakes! E.g., in the discussion, it says there is no significant difference between VAS scores between the two groups. However, in the results it says there was a significant difference with regard to VAS scores for leg pain which was lower in the open discectomy group. here is another example: check out this verbiage: “one patient, who was free of complaints after a failed laser discectomy…” A failed discectomy means the patient continues to have complaints, so which is it? And finally, as mentioned above, what happened to the 44% of the patients who underwent "surgery," with regard to clinical outcomes? Those failures have to be counted against laser discectomy, yet the results say that functional outcomes were the same between the groups. This doesn't make sense. Personally, I'm super surprised this paper was allowed in such a prestigious spine Journal… I don't get it?
Note: I just discovered a few other researchers who are irritated by this paper's publication. They even wrote a formal attack of this paper which you can read for free at this link: paper gets attacked
MINIMALLY INVASIVE VERSUS OPEN TRANSFORAMINAL LUMBAR INTERBODY FUSION: WHICH ONE DECREASES THE CHANCES OF NEEDING A SECOND SURGERY IN THE NEAR FUTURE?
Galetta, M. S., et al. “Reoperation Rates Due To Adjacent Segment Disease Following Primary 1 or 2-Level Minimally Invasive Versus Open Transforaminal Lumbar Interbody Fusion.” SPINE: 2023; 48(18)P1295-1299.
In September, 2023, Galetta et al. published the results of their retrospective study in the prestigious Journal, Spine.The abstract of the paper, which is what most people see online (most folks can not afford to buy these expensive papers and read/understand all the details), reported the results of “238” patients who had undergone either open TLIF or minimally invasive TLIF.
Surprisingly (at least to me), at the three-year after-surgery evaluation, they found patients undergoing traditional open TLIF had a 23.2% reoperation rate (i.e., revision rate. They needed another surgery because the pain returned), versus an 8% reoperation rate for the MIS-TLIF group! This result was statistically significant (p=0.03).
I could not believe this result, for anatomically, biomechanically, and physiologically it just didn't make sense to me. So I obtained the full paper and read the details.
I WAS SHOCKED THAT THIS PAPER WAS EVEN LET INTO THE PRESTIGIOUS SPINE!
Here’s what I found, which really cast doubt on the study's conclusions:
#1) there is a major error reported in the results: “in total 238 patients underwent TLIF…” ...189 underwent MIS-TLIF and 259 underwent open-TLIF. If you add 189 + 259, that comes to 448! So which is it? was the study made of 238 patients OR 448 patients? Huge mistake! How could such an error get by the SPINE editor?
BUT HERE'S THE MOST SHOCKING FINDING!
#2) at the three-year follow-up examination, the “lost to follow-up rate” (i.e., the number of patients they couldn’t get a hold of to re-examine at three years) was 50.5% for the MIS-TLIF group and 46.2% for the Open-TLIF group!!! What the F****!
It is well known that a spine research paper should not be published when more than 20% of the patients studied cannot be rounded up for the follow-up exam! This is because a loss greater than that will make the paper's conclusions statistically insignificant and unreliable.
So, in this paper, about half of the patients in each group disappeared and were not available for follow-up!
Therefore, the results of this study are completely worthless, for we don't know the conditions of these patients. Maybe they had surgery at another clinic? Maybe some died? We just don't know!
How in the world did this get published in spine! I have been published in this once-prestigious spine Journal and can tell you firsthand that it used to be extremely difficult to get papers published here. Apparently, not anymore!
The even more scary thing is that if you only read the free abstract, which most doctors / laypeople do, you would have thought that the patient needs a minimally invasive form of TLIF (which I never recommend in my coachingService)and not the time-tested open TLIF procedure. The only way you would have caught the truth is if you bought the paper and read the details for yourself!
I am very very disappointed in the publication of this paper, which definitely gives this once-prestigious spine journal a blackeye!
DOES MICRODISCECTOMY INCREASE YOUR CHANCE OF RETURNING TO SPORT AFTER SYMPTOMATIC DISC HERNIATION?
I looked at two high-quality meta--analyses in attempts to answer this question. Let's see what they have to say:
Overly SC, et al. Return to Play Elite Athletes after Lumber My Discectomy a Meta-Analysis: SPINE: 2016;41(8):713-8.
In this meta-analysis, after looking at 547 articles on the subject, Overly et al pooled together the data from 14 high-quality studies in order to answer the question, “what are the chances of an elite athlete returning to play after undergoing a microdiscectomy.”
Conclusion: they discovered that 83.5% of them did return to play/sport after undergoing a single level microdiscectomy. Surprisingly, they also discovered that just as many return to play/sport after choosing not to have a microdiscectomy!
Therefore, this study would suggest that discectomy does not improve your chances at returning to play/support.
In Sedrak P, et al's "Return to Play after Symptomatic Lumbar Disc Herniation in Elite Athletes: a Systematic Review and Meta-Analysis of Operative Versus Nonoperative Treatment," they found about the same thing: having had a microdiscectomy appears not to be a predictor of whether or not you can return to sport/play.
Here's the bottom line: After pooling together 799 patients, this group of researchers found basically the same thing that Overly did: 83.0% returned to play in the surgical group. 81.5% returned to play in the nonoperative group. The nonoperative group, however, returned to play faster (four months versus five months.
COMMENTS: I think one of the problems here was that small contained disc herniations, which probably shouldn't of been operated on anyway, skewed the results of the study. It would be interesting to see the results of discectomy performed only on moderate or large sized herniations. I bet things would change?
OH NO! ANOTHER HIGH-INTENSITY ZONE PAPER! A SINGLE LEVEL HIZ IS NOT PREDICTIVE OF LOW BACK PAIN OR SCIATICA
Teraguchi et al. “Lumbar High-Intensity Zone on MRI: imaging biomarkers for severe, prolonged low back pain and sciatica in a population-based cohort. Spine J 2020;20(7): 1025 – 1034. [review written 9/28/20]
Early this year (2020), Teraguchi et al. published the largest investigation to date which looked at the phenomenon of high-intensity zone (HIZ) and its relationship to chronic back pain and sciatica (radicular pain). This was a follow-up study to his systematic review of 2018 which suggested HIZ was related to chronic low back pain but the evidence was mixed and a larger, better design study was needed.
BOTTOM LINE
In my mind, this study continues the confusion about HIZ, for although the results of this large study demonstrated that multilevel homogeneous (same type of tears) posterior HIZs were predictive of chronic back pain and sciatica (p <0.02), they were not predictive of disability levels.
Surprisingly, risk factors that are known to damage the disc (i.e., high BMIs, smoking, and heavy lifting occupations) were also not associated with HIZ.
I have some serious concerns with the study data, some of which is flat out unbelievable. For example, according to table #1, over 40% of the people in the study had ODIs scores over 60%! Us researchers who are also clinicians know that an ODI of that magnitude means the person is severely disabled and could not work. Certainly, 40% of this Japanese population are not severely disabled? It must be a typo, but it makes you wonder how many other errors are in this research paper?
Table II also said that ODI was predictive of the presence of HIZ (p<0.05), which disagrees with the verbiage of the paper which said that HIZ had no relationship to ODI score. Must also be another typo.
So this paper definitely must be taken with a grain of salt.
The only thing you can really say is that if someone has multilevel (2 or more discs) homogeneous annular tears on T2-weighted MRI, they probably have a history of significant bouts of low back pain and possibly sciatica.
INTRODUCTION
Since Aprill and Bogduk first introduced the theory that HIZ was associated with chronic pain in 1992, controversy has swirled around the issue. Plenty of studies have found a relationship between HIZ and chronic pain, while plenty have not.
In hopes of shedding more light on the matter, this team of researchers put together the largest study to date on HIZ and its relationship to back pain.
SET-UP
Painstakingly, a slice of the general population was gathered for evaluation. They were not specifically looking for low back patients. They invited everybody to participate in the study and didn’t even mention it was for assessing low back pain. They were able to gather 1414 subjects. The average age was of the study group was 48 years, and there were 63% female and 37% male.
The subjects then completed a questionnaire with regard to their low back and leg. Specifically, how often did they have attacks of low back pain, if ever? How severe was the low back pain? (“Severe” low back pain was defined as an attack lasting longer than 30 days and/or 6/10 on VAS) Do they have radicular pain and was it associated with their low back pain? What is the weight? How heavy is their occupation? Do they smoke? Data with regard to current medical conditions is also gathered.
After the data was obtained, 200 of the subjects were kicked out of the study (excluded) for having conditions like history of prior spine surgery, inflammatory conditions, metabolic disease, significant spinal deformities (scoliosis). The remaining 1214 subjects were enrolled in the study and then had a three Tesla MRI to look for signs of HIZ, degenerative disc disease, Modic change, disc bulges, and disc herniations. Strangely, board certified orthopedic surgeons were used to interpret imaging results and not radiologists.
RESULTS
^ 59% (718) of all patients had at least one HIZ which was located posteriorly by far (50.7%). Of the 718 patients, most had a single level HIZ (53.3%) or double level HIZ (32.5%). 13% had three or four HIZs. Note: the Wakayama study found a prevalence of 38% in a group of 814 Japanese subjects.
^Older patients had significantly more chance of having an HIZ that younger patients (p<0.0001)
^ ^ surprisingly, BMI, heavy smokers, and heavy laborers did not have an increased risk of developing HIZ!
^ ^ Patients with two or more HIZs had significantly more disc degeneration (p<0.001)
^ patients with HIZ more commonly had a history of prolonged severe low back pain and suffered more frequent attacks of this pain (p<0.011)
^ ^ Single-level HIZ did not demonstrate significant risk for prolonged severe low back pain or sciatica.
^ ^ Multilevel anterior HIZs or a mix of anterior posterior HIZs were not associated with prolonged severe low back pain.
^ This was the first study to note that multilevel homogeneous HIZs were significantly and independently associated with prolonged severe low back pain and sciatica.
CONCLUSION
Even though this study was published in a high-impact spine Journal, The Spine Journal, it has some unbelievable data. For example, it said that 41% of the general population who entered this study has a severe disability as noted by an ODI score of over 60%. That’s absurd!
Table II also said that ODI was predictive of HIZ (p<0.05), yet the main paper said it wasn’t. So which is it?
Really disappointed that I wasted my time reading this! I thought it was safe because it was in a high-impact spine Journal, but the subject entry data is unbelievable with regard to their level of disability. For me, it makes me wonder how many other mistakes there are in this paper.
Nevertheless, it seems that having multiple homogeneous annular tear is predictive of someone having a bad back and possibly sciatica.
I did email the authors to see what their response was with regard to the table errors, but I doubt if I’ll get a response. If I do, I will amend this review accordingly.
Kilpikoski s, Hakkinen A, et al. “The McKenzie Method versus Guideline-based Advice in the Treatment of Sciatica: 24-Month Outcomes of a Randomized Clinical Trial.” Clinical rehabilitation (impact factor 2.9); 2024; 38:72-84.
 Physical therapists have been touting the efficacy and effectiveness of McKenzie Exercises (McKenzie method) for years as an effective treatment for sciatica.
Physical therapists have been touting the efficacy and effectiveness of McKenzie Exercises (McKenzie method) for years as an effective treatment for sciatica.
Anecdotally, however, I have found these extension movements not helpful for patients with true disc-herniation-induced and/or stenosis-induced sciatica. In fact, in some cases, it has made the problem worse, as confirmed in this study (7% got worse from these treatments).
This morning, I stumbled across a 2024 randomized controlled clinical trial that supports my hypotheses that these exercises are not effective for disc herniation-induced or stenosis-induced sciatica.
Specifically, in 2024, Clinical Rehabilitation (impact factor, 2.9 {a very well respected, peer-reviewed medical Journal}) published an article by Kilpikoski et al. (Finland) which demonstrated that the McKenzie method/exercises (doing these exercises/movements in clinic and at home) (as performed by a very experienced McKenzie certified physical therapist {at least 15 years experience}) were no more effective in the long run (24 months) at reducing pain and disability from sciatica, compared to one 90 minute instructional session with the physical therapist.
It should be noted that both groups improved equally well with regard to pain (VAS) and disability (i.e., the ability to perform the activities of daily living (ODI)); furthermore, this improvement did reach a level of significance (p<0.05) when compared to baseline scores.
It should be also that nobody in the control group was hurt and knocked out of the study. On the other hand, 7% of the McKenzie group suffered “adverse events” which ended the therapy.
To me, it never made sense to put someone with a posterior lumbar disc herniation into extension, which will compress the posterior part of the disc (the part that's torn open) and possibly make it poke out farther or even rupture. Extension also causes stenosis of the vertebral canal, which would also increase the effective magnitude of the herniations volume in the vertebral canal.
MINIMALLY INVASIVE VERSUS OPEN TRANSFORAMINAL LUMBAR INTERBODY FUSION: WHICH ONE DECREASES THE CHANCES OF NEEDING A SECOND SURGERY IN THE NEAR FUTURE?
Galetta, M. S., et al. “Reoperation Rates Due To Adjacent Segment Disease Following Primary 1 or 2-Level Minimally Invasive Versus Open Transforaminal Lumbar Interbody Fusion.” SPINE: 2023; 48(18)P1295-1299.
In September, 2023, Galetta et al. published the results of their retrospective study in the prestigious Journal, Spine.The abstract of the paper, which is what most people see online (most folks can not afford to buy these expensive papers and read/understand all the details), reported the results of “238” patients who had undergone either open TLIF or minimally invasive TLIF.
Surprisingly (at least to me), at the three-year after-surgery evaluation, they found patients undergoing traditional open TLIF had a 23.2% reoperation rate (i.e., revision rate. They needed another surgery because the pain returned), versus an 8% reoperation rate for the MIS-TLIF group! This result was statistically significant (p=0.03).
I could not believe this result, for anatomically, biomechanically, and physiologically it just didn't make sense to me. So I obtained the full paper and read the details.
I WAS SHOCKED THAT THIS PAPER WAS EVEN LET INTO THE PRESTIGIOUS SPINE!
Here’s what I found, which really cast doubt on the study's conclusions:
#1) there is a major error reported in the results: “in total 238 patients underwent TLIF…” ...189 underwent MIS-TLIF and 259 underwent open-TLIF. If you add 189 + 259, that comes to 448! So which is it? was the study made of 238 patients OR 448 patients? Huge mistake! How could such an error get by the SPINE editor?
BUT HERE'S THE MOST SHOCKING FINDING!
#2) at the three-year follow-up examination, the “lost to follow-up rate” (i.e., the number of patients they couldn’t get a hold of to re-examine at three years) was 50.5% for the MIS-TLIF group and 46.2% for the Open-TLIF group!!! What the F****!
It is well known that a spine research paper should not be published when more than 20% of the patients studied cannot be rounded up for the follow-up exam! This is because a loss greater than that will make the paper's conclusions statistically insignificant and unreliable.
So, in this paper, about half of the patients in each group disappeared and were not available for follow-up!
Therefore, the results of this study are completely worthless, for we don't know the conditions of these patients. Maybe they had surgery at another clinic? Maybe some died? We just don't know!
How in the world did this get published in spine! I have been published in this once-prestigious spine Journal and can tell you firsthand that it used to be extremely difficult to get papers published here. Apparently, not anymore!
The even more scary thing is that if you only read the free abstract, which most doctors / laypeople do, you would have thought that the patient needs a minimally invasive form of TLIF (which I never recommend in my coachingService)and not the time-tested open TLIF procedure. The only way you would have caught the truth is if you bought the paper and read the details for yourself!
I am very very disappointed in the publication of this paper, which definitely gives this once-prestigious spine journal a blackeye!
DOES MICRODISCECTOMY INCREASE YOUR CHANCE OF RETURNING TO SPORT AFTER SYMPTOMATIC DISC HERNIATION?
I looked at two high-quality meta--analyses in attempts to answer this question. Let's see what they have to say:
Overly SC, et al. Return to Play Elite Athletes after Lumber My Discectomy a Meta-Analysis: SPINE: 2016;41(8):713-8.
In this meta-analysis, after looking at 547 articles on the subject, Overly et al pooled together the data from 14 high-quality studies in order to answer the question, “what are the chances of an elite athlete returning to play after undergoing a microdiscectomy.”
Conclusion: they discovered that 83.5% of them did return to play/sport after undergoing a single level microdiscectomy. Surprisingly, they also discovered that just as many return to play/sport after choosing not to have a microdiscectomy!
Therefore, this study would suggest that discectomy does not improve your chances at returning to play/support.
In Sedrak P, et al's "Return to Play after Symptomatic Lumbar Disc Herniation in Elite Athletes: a Systematic Review and Meta-Analysis of Operative Versus Nonoperative Treatment," they found about the same thing: having had a microdiscectomy appears not to be a predictor of whether or not you can return to sport/play.
Here's the bottom line: After pooling together 799 patients, this group of researchers found basically the same thing that Overly did: 83.0% returned to play in the surgical group. 81.5% returned to play in the nonoperative group. The nonoperative group, however, returned to play faster (four months versus five months.
COMMENTS: I think one of the problems here was that small contained disc herniations, which probably shouldn't of been operated on anyway, skewed the results of the study. It would be interesting to see the results of discectomy performed only on moderate or large sized herniations. I bet things would change?
OH NO! ANOTHER HIGH-INTENSITY ZONE PAPER! A SINGLE LEVEL HIZ IS NOT PREDICTIVE OF LOW BACK PAIN OR SCIATICA
Teraguchi et al. “Lumbar High-Intensity Zone on MRI: imaging biomarkers for severe, prolonged low back pain and sciatica in a population-based cohort. Spine J 2020;20(7): 1025 – 1034. [review written 9/28/20]
Early this year (2020), Teraguchi et al. published the largest investigation to date which looked at the phenomenon of high-intensity zone (HIZ) and its relationship to chronic back pain and sciatica (radicular pain). This was a follow-up study to his systematic review of 2018 which suggested HIZ was related to chronic low back pain but the evidence was mixed and a larger, better design study was needed.
BOTTOM LINE
In my mind, this study continues the confusion about HIZ, for although the results of this large study demonstrated that multilevel homogeneous (same type of tears) posterior HIZs were predictive of chronic back pain and sciatica (p <0.02), they were not predictive of disability levels.
Surprisingly, risk factors that are known to damage the disc (i.e., high BMIs, smoking, and heavy lifting occupations) were also not associated with HIZ.
I have some serious concerns with the study data, some of which is flat out unbelievable. For example, according to table #1, over 40% of the people in the study had ODIs scores over 60%! Us researchers who are also clinicians know that an ODI of that magnitude means the person is severely disabled and could not work. Certainly, 40% of this Japanese population are not severely disabled? It must be a typo, but it makes you wonder how many other errors are in this research paper?
Table II also said that ODI was predictive of the presence of HIZ (p<0.05), which disagrees with the verbiage of the paper which said that HIZ had no relationship to ODI score. Must also be another typo.
So this paper definitely must be taken with a grain of salt.
The only thing you can really say is that if someone has multilevel (2 or more discs) homogeneous annular tears on T2-weighted MRI, they probably have a history of significant bouts of low back pain and possibly sciatica.
INTRODUCTION
Since Aprill and Bogduk first introduced the theory that HIZ was associated with chronic pain in 1992, controversy has swirled around the issue. Plenty of studies have found a relationship between HIZ and chronic pain, while plenty have not.
In hopes of shedding more light on the matter, this team of researchers put together the largest study to date on HIZ and its relationship to back pain.
SET-UP
Painstakingly, a slice of the general population was gathered for evaluation. They were not specifically looking for low back patients. They invited everybody to participate in the study and didn’t even mention it was for assessing low back pain. They were able to gather 1414 subjects. The average age was of the study group was 48 years, and there were 63% female and 37% male.
The subjects then completed a questionnaire with regard to their low back and leg. Specifically, how often did they have attacks of low back pain, if ever? How severe was the low back pain? (“Severe” low back pain was defined as an attack lasting longer than 30 days and/or 6/10 on VAS) Do they have radicular pain and was it associated with their low back pain? What is the weight? How heavy is their occupation? Do they smoke? Data with regard to current medical conditions is also gathered.
After the data was obtained, 200 of the subjects were kicked out of the study (excluded) for having conditions like history of prior spine surgery, inflammatory conditions, metabolic disease, significant spinal deformities (scoliosis). The remaining 1214 subjects were enrolled in the study and then had a three Tesla MRI to look for signs of HIZ, degenerative disc disease, Modic change, disc bulges, and disc herniations. Strangely, board certified orthopedic surgeons were used to interpret imaging results and not radiologists.
RESULTS
^ 59% (718) of all patients had at least one HIZ which was located posteriorly by far (50.7%). Of the 718 patients, most had a single level HIZ (53.3%) or double level HIZ (32.5%). 13% had three or four HIZs. Note: the Wakayama study found a prevalence of 38% in a group of 814 Japanese subjects.
^Older patients had significantly more chance of having an HIZ that younger patients (p<0.0001)
^ ^ surprisingly, BMI, heavy smokers, and heavy laborers did not have an increased risk of developing HIZ!
^ ^ Patients with two or more HIZs had significantly more disc degeneration (p<0.001)
^ patients with HIZ more commonly had a history of prolonged severe low back pain and suffered more frequent attacks of this pain (p<0.011)
^ ^ Single-level HIZ did not demonstrate significant risk for prolonged severe low back pain or sciatica.
^ ^ Multilevel anterior HIZs or a mix of anterior posterior HIZs were not associated with prolonged severe low back pain.
^ This was the first study to note that multilevel homogeneous HIZs were significantly and independently associated with prolonged severe low back pain and sciatica.
CONCLUSION
Even though this study was published in a high-impact spine Journal, The Spine Journal, it has some unbelievable data. For example, it said that 41% of the general population who entered this study has a severe disability as noted by an ODI score of over 60%. That’s absurd!
Table II also said that ODI was predictive of HIZ (p<0.05), yet the main paper said it wasn’t. So which is it?
Really disappointed that I wasted my time reading this! I thought it was safe because it was in a high-impact spine Journal, but the subject entry data is unbelievable with regard to their level of disability. For me, it makes me wonder how many other mistakes there are in this paper.
Nevertheless, it seems that having multiple homogeneous annular tear is predictive of someone having a bad back and possibly sciatica.
I did email the authors to see what their response was with regard to the table errors, but I doubt if I’ll get a response. If I do, I will amend this review accordingly.