
Discogenic Pain Syndrome (aka: Internal disc disruption)
General | History | How Does it Occur? | How Does It Become Painful? | The Research | The Diagnosis | The Tutorial | Treatment Options
Discogenic Pain Syndrome: General Stuff
 Just because that disc of yours looked normal on MRI, does not mean that it can't to be causing your chronic back pain. This is because that innocent looking disc, especially if it is black in color (i.e., degenerated), [132] may be harboring a pain-generating "tear" inside of it. These tears, which are called and these "annular tears," have the capability to produce agonizing chronic low back pain which his referred to as a Discogenic Pain Syndrome (or, in layman's terms, "torn-disc-related back pain").
Just because that disc of yours looked normal on MRI, does not mean that it can't to be causing your chronic back pain. This is because that innocent looking disc, especially if it is black in color (i.e., degenerated), [132] may be harboring a pain-generating "tear" inside of it. These tears, which are called and these "annular tears," have the capability to produce agonizing chronic low back pain which his referred to as a Discogenic Pain Syndrome (or, in layman's terms, "torn-disc-related back pain").
As the name implies, discogenic pain is a pain that arises from the disc itself, secondary to tears within the annulus fibrosus. I have covered these tears in detail on the annular tear page, so some of this is going to be overlap. However, I will focus more on the clinical aspects of the symptomatic annular tear.
Why hasn't my doctor mentioned discogenic pain syndrome as possible cause of my chronic low back pain? More likely than not, he or she is not familiar with it.
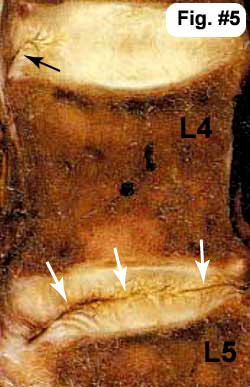
Fig.#5 The white arrows are pointing to a full thickness annular tear (or an internally disrupedt disc) within the L4/5 disc that in this case completely bisects the disc (there are many different flavors of annular tear– see the annular tear page). Note also that the disc above (the L3/4 disc) has a small tear in the outer fibers of the annulus (black arrow) that has not made it (yet) into the middle of the disc. This type of tear is called a 'rim lesion'.
The History of Discogenic Pain Syndrome:
IDD was first described by Crock in 1970 (8) and again in 1986 (9). Specifically, it was then described as a ‘disruption' of the internal architecture of the disc without signs of disc protrusions or without positive signs for nerve root compression’.
In his 1986 presidential address, Dr. H. V. Crock told members of the international spine society that internal disruptions within the architecture of the disc could result in back pain and even lower limb pain without the presence of spinal nerve root compression (9). He termed this entity ‘ Internal Disc Disruption ’ or IDD.
In 1995, a 'Dream Team' of well respected and Volvo Winning researchers (Schwarzer, Aprill, Derby, Bogduk) set out to test and further develop Crock’s theory of IDD and convincingly calculated the prevalence (frequency) of IDD in patients with chronic low back pain. (2) The study also attempted to determine if traditional examination findings and/or specific patient symptoms could be predictive of the diagnosis of IDD. By following the strict criteria specified by the ‘International Society for the Study of Pain in its taxonomy’ (21), these investigators calculated the prevalence of IDD to be between 30% and 50% with a 95% confidence limit. They also concluded that neither traditional examination findings nor patient symptoms could predict whether or not a patient had IDD. Unfortunately, it looks like the controversy over diagnostic procedure, provocation discography, remains the only way to confirm the diagnosis of IDD.
Prevalence of Discogenic Pain Syndrome:
What is the "prevalence" (how often does it occur within the population) of discogenic low back pain ? Although there is not an overabundance of research on the subject, one landmark paper demonstrated that 30% to 50% of people with chronic low back pain suffered from these disc tears, a condition which is also called internal disc disruption (IDD).[2]
Are Annular Tear Always Painful?
Before I continue, it's very important to understand that not all cases of internal disc disruption cause chronic low back pain, and the mechanisms that make some annular tears symptomatic and others not, remains elusive. I personally believe it has something to do with the individual's unique immune system and its ability to generate an inflammatory response. Nevertheless, in some circles discogenic pain syndrome is still a fairly controversial diagnosis. However, the majority of spine specialists and spine researchers (including me) are convinced of its existence. Among supporters is Nikolai Bogduk, MD, who some call the "God" of lumbar anatomy and disease, because of his lifelong study of the lumbar spine, his numerous articles and books, and his numerous awards (including a Volvo Award).
Is the diagnosis of internal disc disruption new? No. In fact it has been around for at least 50 years! Specifically, it was a surgeon/researcher named H.V. Crock who first brought it into the limelight in 1986 by telling told members of the International Spine Society that 'internal disruptions' within the architecture of the disc could result in Not only back, but also lower limb pain (sciatica) without evidence for nerve root compression. [9] He is the one who coined the term internal disc disruption.
Pathophysiology: How Does Discogenic Pain Syndrome Occur?
Discogenic pain syndrome occurs when the posterior annulus (whose job is to hold the highly pressurized nucleus pulposus in the center of the disc) tears (usually from the inside out) through which in turn allows nucleus pulposus to escape from the confines of the disc's center and push into the outer, highly innervated (filled with pain-generated nerve fiber) region of the annulus fibrosus.
How does the tear start in the first place? It is believed that these tears develop from (#1) arduous activity, such as engaging in a heavy/physical job, or participating in heavy contact sports; (#2) severe single-event trauma (e.g., a motor vehicle accident or a slip and fall); and / or (#3) just with the normal wear-and-tear of activities of daily living in patients who have a genetic predisposition for tearing (i.e., the annulus was built with faulty/weak material that is quite easily torn and/or the disc is significantly degenerated).
In order to understand how IDD may cause pain, you will need to know some basis disc anatomy. If you are a little shaky on disc anatomy, please visit my Disc Anatomy Page.
Quick Disc Anatomy Review
 Fig.#4 demonstrates the normal lumbar disc anatomy: Here, in this over-head view, we have the nucleus pulposus (pink) surrounded by the the stronger annulus fibrosus (green). Normally, the annulus fibrosus is strong enough to contain or corral the pressurized nucleus pulposus and keep it from escaping (squirting) outward. Of particular interest to the upcoming discussion are the tiny 'Sinuvertebral Nerves Endings' (yellow poke-a-dots). These tiny nerve fibers, which are embedded within the posterolateral substance of the outer 1/3 of the annulus fibrosus, are known to both initiate and carry the perception of pain into the spinal cord. From there, these pain signals are carried upward to the sensory cortex of the brain. (386-388, 439).
Fig.#4 demonstrates the normal lumbar disc anatomy: Here, in this over-head view, we have the nucleus pulposus (pink) surrounded by the the stronger annulus fibrosus (green). Normally, the annulus fibrosus is strong enough to contain or corral the pressurized nucleus pulposus and keep it from escaping (squirting) outward. Of particular interest to the upcoming discussion are the tiny 'Sinuvertebral Nerves Endings' (yellow poke-a-dots). These tiny nerve fibers, which are embedded within the posterolateral substance of the outer 1/3 of the annulus fibrosus, are known to both initiate and carry the perception of pain into the spinal cord. From there, these pain signals are carried upward to the sensory cortex of the brain. (386-388, 439).
ADVANCED: The pain pathways (how the degenerated disc tissue pain gets from the disc to the brain) for discogenic pain are still very controversial and may not function as traditional anatomy has taught us. Traditionally, pain signals that originate in the nerve roots adjacent to the disc or within the disc itself move from that root, into the corresponding DRG and then into the spinal cord. However, some new research suggests that pain signals from the lower lumbar discs (L5 and L4) are (at least in part) detoured up the sympathetic nerves (i.e., gray ramus communicans) and into the upper lumbar DRGs - especially at the L2 level. (11, 259, 260) Clinically, in some patients it then would be possible for patients with L4 and L5 disc problems to have L1 or L2 dermatomal pain (groin and anterior thigh pain).
How & When Does An Annular Disc Tear Become Painful?
First, in order to become painful, the annulus fibrosus must rip open and allow nucleus pulposus material to enter the outer one third of the disc. Why does the annulus fibrosus rip open? One group of researchers believe that it occurs in part secondary to a buildup of pressure within the nucleus pulposus. But what causes the pressure buildup?
Onik et al [304] explained that the intervertebral disc may be considered an osmotic system, secondary to the breakdown of disc macromolecules during the fourth and fifth decades of life. The splitting apart of these large molecules results in an increased number of particles which results in an increased "sucking force" within the nucleus and annulus. In other words, more water is sucked into the disc which in turn raises the osmotic pressure. This pressure actually is thought to rip the annulus fibrosus in people who are susceptible (have poor genetics for disc building materials) and an annular fissure develops which then may go on to become painful.
okay, the disc is ripped, but how does it become painful?
In order for the tear to become painful, it must have ripped into the posterior one-third of the disc, which of course (I hope you studied your disc anatomy) is where the pain-carrying nerve fibers of the sinuvertebral nerves live. Although controversy, the exact mechanism of pain is two-pronged:
#1) it is believed that "evil" pro-inflammatory biochemicals (like the cytokines TNF-a, IL-1, IL-6), which are known to occur in high concentrations within degenerated disc tissue, will leak and soak into the nociceptors (pain switches) of the sinuvertebral nerve, which in turn triggered the nociceptors to fire signals of pain to the brain. This is known as a chemical irritation of the nociceptors. Furthermore, now in information can start in the adjacent tissue which in turn perpetuates the irritation of these nociceptors.
#2) The full thickness tear will also destroy the normal biomechanics of the disc which changes the point of maximum weight-bearing from the center of the disc to the posterior part of the disc which is where all these inflamed nociceptors are. So now, every time the patient twists, turns and bends at the waist, the already inflamed and irritated nociceptors are mechanically irritated, which also upsets them and triggers them to send pain impulses to the brain.
Autoimmune Reaction Theory?
There is some evidence that the actual nucleus pulposus cells which leak from the center of the disc into the region of the nociceptors (i.e., outer one third of the posterior and posterolateral disc) results in an autoimmune inflammatory process, because these cells have never been seen by the body's immune system before.
 In Fig. #3 the disc has ripped through or "disrupted" and has allowed nuclear material (pink) to escape into the outer and sensitive 1/3 of disc (i.e. the annulus fibrosis). The sinuvertebral nerves (yellow dots) in contact with this degenerated nuclear material have become inflamed (red dots) and irritated, which in turn causes pain signals to 'fire off' to the dorsal horn of the cord and then to the brain, which causes the patient to feel pain. Some patients even suffer a referred type pain (discogenic sciatica) down the lower limb(s), yet they have no traditional compression of the adjacent nerve roots.
In Fig. #3 the disc has ripped through or "disrupted" and has allowed nuclear material (pink) to escape into the outer and sensitive 1/3 of disc (i.e. the annulus fibrosis). The sinuvertebral nerves (yellow dots) in contact with this degenerated nuclear material have become inflamed (red dots) and irritated, which in turn causes pain signals to 'fire off' to the dorsal horn of the cord and then to the brain, which causes the patient to feel pain. Some patients even suffer a referred type pain (discogenic sciatica) down the lower limb(s), yet they have no traditional compression of the adjacent nerve roots.
Research: The Critics of Internal Disc Disruption
The theory of IDD as a source of chronic back pain is not without its critics. In 2003, Lee et al. reviewed the research on IDD from 1985 through 2000, (10) although the papers review were mostly geared toward radial tears and HIZ. He summarized that of the 13 research papers on IDD, there was not much agreement on what constituted the diagnosis of IDD. What the authors did agree upon, however, was that patients with IDD had concordant low back pain upon provocative discography and a completely normal neurological examination (i.e., there were no deep tendon reflex changes, no loss of sensation, and no muscle atrophy or weakness). Other signs of IDD, which include the MRI presence of a high intensity zone (HIZ), significant disc degeneration (a black disc on MRI), and a history of trauma to the lumbar spine, were not universally agreed upon by the experts.
Based on their review of '15 years worth of research', Lee et al. concluded that “IDD is not real, but a hypothetical disease”. This Korean group further stated the following; “Our personal view is that IDD is a doctor-made disease, that is, an iatrogenic disc disorder, which may lead to an unconventional invasive operations (referring to the IDET procedure and Lumbar Fusion).” [10] Furthermore, Lee felt that because the diagnosis was so dependent upon the 'subjective input' from the patient during discography, that the diagnosis should be thrown out completely!
IMHO: Lee, who is way out of his usual area of research, is going to be criticized for making such aggressive statements against the theory of IDD, which has been accepted by the 'North American Spine Society' (21) and the 'International Society for the Study of Pain in its Taxonomy' (21)! For the typical non-mentally compromised chronic pain patient, the diagnosis of IDD can be made with a reasonable degree of medical certainty by using the criteria that the International Society for the Study of Pain in its Taxonomy have adopted (Here) for the criteria.
Internal Disc Disruption: Other Research
Although controversial (436), discogenic pain secondary to IDD is thought to be responsible for a substantial number of chronic back and leg pain cases where obvious nerve root compression is absent/lacking. [132, 2] In fact the famous multi-time Volvo Award Winning author, professor Nikolai Bogduk MD, believes IDD is the "most common cause of chronic low back pain" (1,2) and may be often over-looked by the treating physician." (132).
Quality scientific research has demonstrated that 30% to 50% of all chronic back pain is caused by the radial annular tears of IDD, [2] and often presents (62% of the time according to Ohnmeiss et al.) as back pain and/or pain down the lower extremity. [6]
The theory on how the annular tears within the annulus cause chronic low back and leg pain remains fairly speculative and contraversial. However, the available research seems to indicate that evil biochemicals called "cytokines" may leak from the degenerated nucleus pulposus onto the nociceptive fiber that lives within the posterior and posterolateral annulus fibrosus, which in turn sets up a vicious cycle of inflammation – pressure buildup – nociceptive stimulation (pain). [105,115,116,123,124,131]
Recently, it has been demonstrated that IDD was the causative factor in about three-quarters of severely acute nonspecific low back pain patients. More explicitly, in 2005 Hyodo et al (16) performed MRIs and discography on 55 patients who all suffered severe, immobilizing, non-specific low back pain without sign of neurological deficit. In 73% of these patients, a full thickness grade 3 or grade 4 annular tear was identified on discography that responded to fluoroscopic lidocaine irrigation (a powerful anesthetic) by instantly 'stopping' the patient's perception of severe pain. (16) The aforementioned experiment strongly advocates that full thickness annular tears – or IDD – are a major cause of severe acute non-specific low back pain.
THE DIAGNOSIS: Discography & Gadolinium-DTPA Enhanced MRI
The 'International Society for the Study of Pain in its taxonomy’ (21) has adapted the following set of criteria for diagnosing IDD: (2,351,352,355)
- There can be no visible disc herniations seen on MRI or CT.
- The patient must experience his usual and customary and/or leg pain (this is called concordant pain) during the injection of contrast into the nucleus pulposus.
- There must be a "control disc." Specifically, after finding a painful disc, they inject the adjacent disc and find that it does not cause concordant pain or any pain at all.
- There must be a grade 3 or grade 4 radial annular tear present, as viewed on CT follow-up or fluoroscopy.
 Provocation discography, which may actually further damage the disc, should ONLY be attempted if the chronic pain patient can no longer live with their pain syndrome and is contemplating IDET, SED, DiscTRODE, interbody spinal fusion or ADR. Furthermore, their Oswestry better be at least a 50! (Oswestry)
Provocation discography, which may actually further damage the disc, should ONLY be attempted if the chronic pain patient can no longer live with their pain syndrome and is contemplating IDET, SED, DiscTRODE, interbody spinal fusion or ADR. Furthermore, their Oswestry better be at least a 50! (Oswestry)
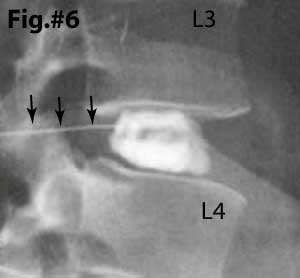
The 'Gold Standard' in making the diagnosis of IDD is a very painful and invasive test called 'Provocation Discography' with follow-up CT discogram. There are two components to provocation discography: the first is an attempt by the doctor to 'provoke' or 'cause' the patient to feel their 'usual' pain (concordant pain) by pressurizing the disc with a contrast material. Note: in Fig.#6 the center of the disc is being filled with contrast material (white). If you look closely, you can see the fine 'white' needle (black arrows) entering the posterior of the disc. This (fig. #6) represents a normal disc that 'holds' the dye within the nucleus and does not demonstrate any anular tearing.
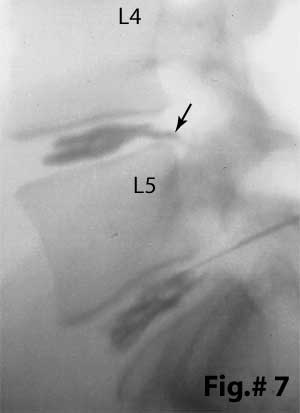 Fig.#7, on the other hand, demonstrates two completely disrupted discs: The contrast material (black in this photo) has NOT been contained within the center (nucleus) of the disc. This time, it has clearly leaked through internal 'disruptions' within the posterior annulus of the L4/5 and L5/S1 disc. In fact, the L4/5 disc has been completely disrupted and it leaking contrast material directly into the epidural space (black arrow). The latter situation is called a Grade 5 anular tear or Grade 5 IDD. (learn about the Dallas discogram naming system and the different degrees of disc disruption here about half way down the page.) This situation may indicate big trouble, especially if you are one of unfortunates who are 'sensitive' (allergic) to those leaking biochemicals (cytokines), for the delicate posterior neural structures 'dwell' adjacent to the posterior of the disc and may become inflamed and/or damaged from this leakage. More explicitly, substance like TNF-alpha, IL-1, IL-6, NO, Phospholipase A1 may stimulate some form of 'attack' within the nerve root and ultimately lead to permanent nerve (axon) death. Neuropathic pain may be spawned.
Fig.#7, on the other hand, demonstrates two completely disrupted discs: The contrast material (black in this photo) has NOT been contained within the center (nucleus) of the disc. This time, it has clearly leaked through internal 'disruptions' within the posterior annulus of the L4/5 and L5/S1 disc. In fact, the L4/5 disc has been completely disrupted and it leaking contrast material directly into the epidural space (black arrow). The latter situation is called a Grade 5 anular tear or Grade 5 IDD. (learn about the Dallas discogram naming system and the different degrees of disc disruption here about half way down the page.) This situation may indicate big trouble, especially if you are one of unfortunates who are 'sensitive' (allergic) to those leaking biochemicals (cytokines), for the delicate posterior neural structures 'dwell' adjacent to the posterior of the disc and may become inflamed and/or damaged from this leakage. More explicitly, substance like TNF-alpha, IL-1, IL-6, NO, Phospholipase A1 may stimulate some form of 'attack' within the nerve root and ultimately lead to permanent nerve (axon) death. Neuropathic pain may be spawned.
Although provocation discography with CT discography is the "gold standard" when it comes to making the diagnosis of symptomatic IDD, the procedure itself can inflict damage upon the disc and "spawn" degenerative disc disease (30-34,530). As an alternative, the use of gadolinium (contrast) enhancement may be considered. Gadolinium-DTPA, which is injected into the blood stream during the MRI, will "light-up" the granulation tissue that forms within a healing/healed full thickness annular disc tear.
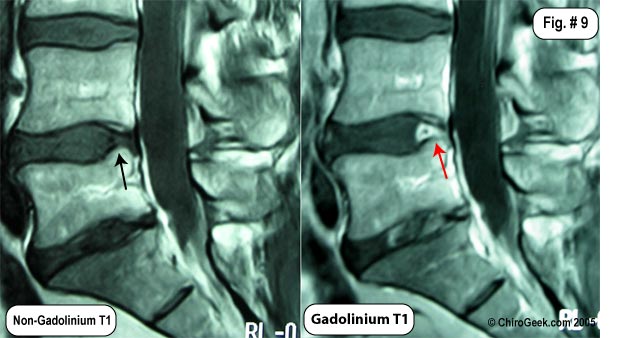 Fig.# 9: The MRI images to the left demonstrates how gadolinium will "light-up" a healed anular tear. Note the L4 disc shows no sign of posterior disc tearing (black arrow); however, after the administration of gadolinium during the MRI, the same T1 image demonstrates the remains of the massive annular tear (red arrow) I suffered back in 2002.
Fig.# 9: The MRI images to the left demonstrates how gadolinium will "light-up" a healed anular tear. Note the L4 disc shows no sign of posterior disc tearing (black arrow); however, after the administration of gadolinium during the MRI, the same T1 image demonstrates the remains of the massive annular tear (red arrow) I suffered back in 2002.
The gadolinium also high-lights continued swelling/granulation tissue within my L5 disc over 1 year post microdiscectomy. No disc herniations are noted.
The HIZ phenomenon also give us a clue that Internal Disc Disruption might be involved in the patients pain syndrome although this T2-weighted MRI finding is highly controversial. For more information, visit my HIZ page.
The Internal Disc Disruption Tutorial
To begin this tutorial, lets look at what a normal disc looks like from the underneath view (axial):
In Figure #4, the basic anatomy of the disc is shown. First note the gelatinous and hydrated nucleus pulposus that is corralled (held in place) by a tough and fibrous annulus fibrosus. The posterior longitudinal ligament (PLL) (blue) is a strong fibrous ligament that courses the entire length of the spine and is tightly bound to the posterior central region of the annulus. It is because of this ligament, that many disc herniations occur in the paracentral region where it is not located.
Particularly important for this tutorial is to note the presence of pain-carrying nerve fiber embedded within the posterior disc. These are called the sinuvertebral nerves and are thought to be responsible for the chronic low back pain associated with annular tears.
It is extremely important to understand that, unlike the rest of the avascular disc, the outer 1/3 of the annulus fibrosus, anterior dura and the PLL are innervated with (full of) tiny nociceptive C-fibers (pain carrying nerve fiber from the sinuvertebral nerves) that, if irritated, have the potential to cause severe PAIN and DISABILITY (4,55,56).
Internal Disc Disruption: How It Typically Occurs
*If you don't understand axial disc anatomy, I strongly recommend that you visit the Disc Anatomy Page in order to get a basic understanding and then returned here—I'm going to assume you know it.
 Typically, the first step in the IDD process is for the disc to become brittle and weak from degenerative disc disease. See the Disc Degeneration Page if you want to learn more about how this degeneration weakens the disc's architecture. (DDD)
Typically, the first step in the IDD process is for the disc to become brittle and weak from degenerative disc disease. See the Disc Degeneration Page if you want to learn more about how this degeneration weakens the disc's architecture. (DDD)
Once such a weakness develops, normal every-day repetitive motions or trauma could start a tear in the inner annulus (figure 2, black arrow. See how a little tear has started at 5 o'clock?).
It is also possible that the tear starts in the outer periphery of the disc secondary to either a concentric annular tear or a rim lesion. [30-34,530]
Figure 2, is a cartoon of a disc that has degenerated, become brittle, and developed both circumferential annular tears (white arrows) and a grade I radial annular tear (black arrow).
Because the radial tear is confined within the inner one-third of the annulus, we called this a grade I annular tear. Grade I annular tears are typically not painful (recall from your disc anatomy lesson that the pain-carrying sinuvertebral nerves are only located in the outer one-third of the annulus) but can develop into a painful full thickness annular tear (a.k.a., grade III) with continued activity or additional trauma.
 In the figure left, the disc has in fact developed a full thickness annular tear (red arrow) which has allowed nucleus pulposus to come in contact with the nociceptive fibers of the sinuvertebral nerves.
In the figure left, the disc has in fact developed a full thickness annular tear (red arrow) which has allowed nucleus pulposus to come in contact with the nociceptive fibers of the sinuvertebral nerves.
How could this full thickness tear be painful? The first reason has to do with biomechanics. As you may recall from the disc anatomy page, when the nucleus is no longer contained to the center, the closed hydraulic system is ruined. Specifically, axial load will now be transmitted directly over the posterior portion of the disc, which is right where the nociceptors are. Therefore, as the theory goes, you get a mechanical irritation of the nociceptors, which in turn creates an inflammatory process (depicted by red nociceptors adjacent to the annular tear). The second reason is because degenerative nuclear material contains some very evil biochemicals called cytokines and others (TNF-alpha, NO, PLA-2, Metalloproteinases, IL-6, PGE-2, Substance-P, Calcitonin gene-related peptide) which now have direct access to the nociceptors, and may start an inflammatory process. Many believe it is this double whammy that creates the horrible low back pain associated with full thickness annular tears of the posterior disc. [287]
*There is also an autoimmune theory, which I happen to be a believer in, that goes like this: because the cells of the nucleus pulposus came to being after birth, and because the nucleus is completely avascular and therefore not exposed to the body's immune system, the cells of the nucleus may be considered foreign. Therefore, if these foreign invaders break out of the nucleus and enter the vascular outer one-third of the  annulus (which is also the location of the nociceptors), the body's the immune system may attack and create an inflammatory reaction in the outer annulus, which in turn will trigger the pain-producing nociceptors.
annulus (which is also the location of the nociceptors), the body's the immune system may attack and create an inflammatory reaction in the outer annulus, which in turn will trigger the pain-producing nociceptors.
Can a full thickness annular tear cause radicular pain (a.k.a., lower extremity pain, or sciatica)?
The short answer is, yes! However, this can only occur if the full thickness annular tear breaks through the final layers of annulus and posterior longitudinal ligament.
Specifically, after the tear completely rips to the disc it could then begins to "drizzle or leak" the evil biochemicals from the disc, onto the adjacent traversing and/or exiting nerve root. (figure 8)
Figure 8 depicts just such a scenario: the full thickness annular tear is now leaking biochemicals, as well as small molecules of nuclear material, which in turn have soaked into the exiting and traversing nerve roots of the sciatic nerve and started a wicked inflammatory process, resulting in radicular pain. This phenomenon, while anecdotally rare, can even cause real radiculopathy (neurological manifestation of symptoms: decreased reflex, decreased sensation, decreased motor power).
Some have called the radicular pain associated with a "leaking disc" discogenic sciatica or discogenic radicular pain.
Discogenic Pain Syndrome: The Available Treatment Options
IDD is a very, very tough condition to treat, especially since the diagnosis is fairly controversial and many primary doctors have never even heard of it before.
Conservative care is ALWAYS the first form of treatment! when I say "conservative care" I mean treatment such as physical therapy and exercise, chiropractic treatment, and acupuncture.
Percutaneous Treatments: there are a number of treatments that claim to be able to "seal" the annular tear (via laser, radiofrequency ablation, etc.) of discogenic pain syndrome, which in turn is supposed to stop the sinuvertebral nerve irritation, which in turn starts the chronic back and/or leg pain.
IDET: The IDET procedure (a.k.a.,intradiscal electrotherapy) has really fallen out of favor with leading clinics because the research just can't agree on whether or not it is efficacious (safe and effective) for the treatment of discogenic pain.
Intradiscal Biacuplasty: this is the more evolve version of the old IDET procedure (uses two needles instead of one) which most likely has a better chance of cauterizing an annular tear shut and relieving pain. There are two big studies out right now and one of them is still ongoing, but the bottom line is that this treatment is not a panacea And should only be used as a last-ditch effort to avoid the end of the road treatment, interbody fusion. I've reviewed the best study we have on biacuplasty to date (9-20-16) right here [Desai-RTC of biacuplasty].
Lumbar Interbody Fusion: If conservative care and percutaneous treatments fail and you are significantly disabled (Oswestry >50), and it is been at least 12 months, then you may start thinking about the "F" word: interbody fusion.
Before you dive into the world of fusion, the evidence-based patient and practitioner will first require that you prove that you are actually suffering from discogenic pain syndrome. Had you do that? Provocation discography!
So, if you're discography testing was positive for concordant pain, then you may consider lumbar interbody fusion.
Warning! Lumbar interbody fusion for the treatment of discogenic pain is very controversial in some circles. This is one of my areas of expertise (I am published in SPINE in this area), and although I do occasionally recommend it, you have to be an absolute perfect candidate!
You can read all about fusion on my fusion page.
References:
1) Bogduk N, McGuirk B, "Pain research and clinical management - Volume 13: Medical management of acute and chronic low back pain." 1st edn. Elsevier - 2002; The Netherlands :119-122
2) Schwarzer AC, Aprill CN, Derby R, Bogduk N, Kine G. “ The prevalence and clinical features of Internal Disc Disruption in patients with Chronic Low Back Pain. ” Spine 1995; 20(17):1878-88
3) Merskey H, Bogduk N, (eds). "Classification of Chronic Pain. Descriptions of Chronic Pain Syndromes and Definitions of pain terms." 2nd edn. IASP Press, Seattle, WA - 1994, pp 180-181
4) Fagan A, "ISSLS Prize Winner: The innervation of the intervertebral disc: A quantitative analysis." Spine - 2003; 28(23):2570-2576
5) Moneta GB, et al "Reported pain during lumbar discography as a function of anular ruptures and disc degeneration: A re-analysis of 833 discograms." Spine 1994; 17:1968-1974
6) Ohnmeiss DD, et al "Degree of disc disruption and lower extremity pain" Spine - 1997; 22(14):1600-1665
7) Luoma, K, et al. "Low back pain in relation to lumbar disc degeneration." Spine - 2000; 25(4):487-92
8) Crock HV, “A reappraisal of intervertebral disc lesions” – Med jour
9) Crock HV, Internal disc disruption. A challenge to disc prolapse fifty years on. Spine 1986 ;11:650-3
10) Lee KS et al. “Diagnostic criteria for the clinical syndrome of IDD” - Brit Jour Neurosurgery 2003; 17(1) 19-23
11) Oh WS, Shim JC. "A randomized Controlled trial of radiofrequency denervation of the ramus communicans nerve for chronic discogenic low back pain." Clin J Pain 2004; 20(1):55-60.
12) Executive Committee of the North American Spine Society. Position statement on discography. Spine 1988; 13:1342
13) Klein RG, Mooney V, Derby RR, et al. "Biochemical injection treatment of discogenic low back pain: a pilot study." The Spine Journal 2003; 3:220-226
14) Mixter WJ, Ayers JB. "herniation or rupture of the intervertebral disc into the spinal canal." N Engl J Med 1935; 213: 385-395.
15) Schellhas KP, et al. “Lumbar Disc High-intensity Zone – MRI & Discography” – Spine 1996; 21:79-86
16) Hyodo H, et al. 'Discogenic Pain in Acute Nonspecific Low-Back Pain' Eur Spine J 2005; Jan 25: On-line ahead of print:1-9.
21) Merskey H, Bogduk N. “Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms.” Seattle: IASP Press, 1994:180-1
30) Osti OL, et al. Volvo Award - "Anulus Tears & Intervertebral Disc Degeneration: an Animal Model" - Spine 1990; 15(8):762-766
31) Moore RJ, Osti OL, Vernon-Roberts B, “Osteoarthrosis of the Facet Joints Resulting From Anular Rim Lesions” – Spine 1999; 24(6):519-524
32) Moore RJ, et al. “Remodeling of Vertebral Bone after Outer Anular Injury in Sheep.” – Spine 1996; 21(8):936-940
33) Key JA, Ford LT “Experimental intervertebral disc lesions” – J Bone Joint Surg 30A:621, 1948
34) Moore RJ et al “Changes in Endplate Vascularity After an Outer Anulus Tear in the Sheep” – Spine 1992; 17(8):874-877
35) Merskey H, Bogduk N. “Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms.” Seattle: IASP Press, 1994:180-1
43) Sachs BL, et al. "Dallas discogram description: a new classification of CT/discography in low-back disorders. Spine - 1987; 12:287-294
44) Aprill C, Bogduk N, "Volvo Award Winner: High intensity zone: a diagnostic sign of painful lumbar disc on MRI." Br J Radiol 1992; 65:361-369
55) Roberts S, et al. "Mechanoreceptors in intervertebral discs: Morphology, distribution, and neuropeptides." Spine - 1995; 20:2645-2651
56) Johnson WE, et al. "Immunohistochemical detection of Schwann cells in innervated and vascularized human intervertebral discs." Spine - 2001; 26:2550-2557
105) Garfin SR, et al. "Compressive neuropathy of spinal nerve roots: A mechanical or biological problem?" Spine - 1991; 16:162-5
115) Marshall LL, et al. "Chemical radiculitis: A clinical, physiological and immunological study." Clin Orthop - 1977:129:61-7
123) Olmarker K, et al. "Ultrastructural changes in spinal nerve roots induced by autologous nucleus pulposus." Spine - 1996; 21:411-4
124) Olmarker K, et al. "Autologous nucleus pulposus induces neurophysiologic and histologic changes in porcine cauda equina nerve roots. " Spine - 1993; 18:1425-32
131) Weinstein J, et al. "The pain of discography." Spine - 1988; 13:1344-8
132) Milette PC, et al. “Radiating Pain to the Lower Extremities Caused by Lumbar Disk Rupture without Spinal Nerve Root Involvement.” AJNR Am J Neuroradiol 1995; 16:1605-1613
259. Morinaga T, Takahashi K, Yamagata M et al. Sensory innervation to the anterior portion of lumbar intervertebral disc. Spine 1996; 21:1848-1851.
260. Ohtori S, Takahashi Y, Takahashi K et al. Sensory innervation of the dorsal portion of the lumbar intervertebral disc in rats. Spine 1999; 24:2295-2299.
287) Rydevik BL. The effects of compression on the physiology of nerve roots. J Manipulative Physiol Ther 1992; 1:62-66.
304) Onik G, et al. “percutaneous lumbar discectomy using a new aspiration probe." AJR 1985; 144:1137 – 1140.
351) Bernard TN. “Lumbar discography followed by computed tomography.” Refining the diagnosis of low-back pain.” Spine 1990; 15:690-707
352) Bogduk N. “The lumbar disc and low back pain.” Neurosurgical Clinics of North America 1991; 2:791-806
353) Crock HV. “Internal disc disruption: A challenge to disc prolapse fifty years on.” Spine 1986; 11:650-653
354) Merskey H, Bogduk N. “Classification of chronic pain. Descriptions of Chronic pain syndromes and Definitions of pain terms.” Seattle: IASP Press, 1994: 180-1
355) Vanharanta H, et al. “A comparison of CT/discography, pain response and radiographic disc height. Spine 1988; 13:321-4
386) Bogduk N et al. “The nerve supply to the human lumbar intervertebral disc.” J Anat 1981; 132:39-56
387) Malinsky J. “The ontogenetic development of nerve terminations in the intervertebral discs of man.” Acta Anat 1959:38:96-113
388) Yoshizawa H et al. “The neuropathology of intervertebral discs removed for low back pain.” 1980 J Pathol; 132:95-104
436) Ross JS, Modic MT, et al. “Tears of the annulus fibrosus: assessment with Gd-DTRA-enhanced MR imaging.” AJNR Am J Neuroradiol 1989; 10:1251-1254
439) McCarty PW, et al. “Immunohistochemical demonstration of sensory fibers and endings in lumbar intervertebral discs of the rat.” Spine 1991; 16:653-655.
530) Kim KS, Yoon ST, Li J, Park JS, Hutton WC. 'Disc degeneration in the rabbit: a biochemical and radiological comparison between four disc injury model s. Spine. 2005 Jan 1;30(1):33-7.
Top | Home
© Copyright Protected - 2002 – 2013- Dr. Douglas M. Gillard DC - All rights reserved