
discography 101
The General Procedure | Is It Safe? | annular tear classification|
Discography: the General Procedure
We have learned on this site that some patients may suffer debilitating back pain and/or leg pain (sciatica) yet have no positive findings on MRI. For these unfortunate patients, the diagnosis of discogenic pain (i.e., the disc itself has become a pain generator) or internal disc derangement (IDD) must be ruled out by a technique called provocative discography. Remember, that the annular tears that give rise to the diagnosis of IDD are often not visible on MRI.
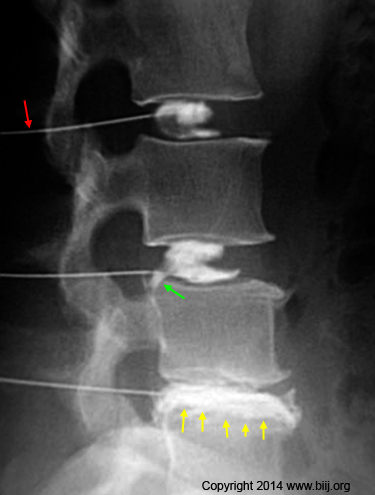
In a nutshell, a needle is carefully inserted into the nucleus pulposus (center of the disc) (red arrow – picture left) under fluoroscopic guidance. Then, contrast is injected into the center of the disc in order to look for "leaks." What would cause a leak? Well, if there is a tear (annular tear) which extends outward from the center of the disc, this tear will now fill with the contrast material and be visible. (Green arrow, yellow arrows).
 Just as important as the visual appearance of full thickness annular tears is whether or not the patient feels pain as contrast is steadily pumped into the nucleus pulposus.
Just as important as the visual appearance of full thickness annular tears is whether or not the patient feels pain as contrast is steadily pumped into the nucleus pulposus.
Specifically, the examiner is supposed to pressurize the contrast-filled disc to 50 psi above the opening pressure (about 70 psi max) and then carefully note whether or not that pressurization re-creates the patient's typical back and/or leg pain. If it does, the patient is said to have had a "concordant pain response" which is indicative of a symptomatic/painful annular tear as the cause of his or her pain syndrome.
To make test even more positive, the examiner will repeat the procedure on at least one adjacent, healthy disc and hopefully get no pain-response from the patient.
And to make the test super positive (i.e., very indicative that the disc is the cause of the low back pain), the examiner can anesthetize the painful disc with lidocaine and repeat the pressurization. This time, the patient should not feel pain since all the nerve endings within the annular tear are now numbed by the lidocaine. This part of the test has recently become a little controversial, for we do know that there are pain-carrying nerve fibers within the subchondral region of the vertebral endplate which may not be affected by the lidocaine bath and still produce pain during the pressurization.
The figure above is a sagittal view (from the side) of the lumbar spine performed via fluoroscopy during discography. Note the needles (red arrow) have been placed in the center of the disc and contrast has been injected. Although the L3 and L4 nucleus are fairly normal (there is a small full thickness tear at L4 {green arrow}), the L5 disc is tore in half and the contrast is certainly not contained (yellow arrows).
The procedure is a true art form and should only be done by the most seasoned of physicians.
Is Discography Safe?
Although the procedure can be incredibly painful (anesthesia is not allowed because the patient-pain response is needed), it is a relatively safe procedure in the short run. However, there is pretty strong evidence that indicates sticking the disc with a needle is not good for the long-term health of the disc.
We know that disc-pokes resulting rapid degeneration of the disc, as well as the creation of full thickness annular tears and even herniations in animals. [5,27-30] In fact, if you want to study degenerative disc disease or annular tears in animals, all you have to do is prick the very outer portion of the annulus with the needle. Such A needle-stick will almost always result in the desired degenerative disc disease and full thickness annular tear within a few weeks.
However, does a needle-stick into a human disc result in the same train of degeneration? The short answer is it appears so, but deleterious effects takes a long time to manifest.
This important question was answered by the famous researcher in spine surgeon, Eugene Carragee of Stanford, who performed an ingenious and award-winning human experiment, which was published in 2009. [1]
In a nutshell, two groups of ~70 people were assembled and matched with regard to sex and age. Both groups underwent MRI to establish a baseline.Then, one group (the study group) underwent provocative discography with conservative techniques, while the other (the control group) did not. Both groups were followed for 10 years and new MRIs were obtained. Although only ~70% of the people in both groups were available at the 10-year follow-up, the results were shocking: there was a statistically significant increase in the frequency of disc herniations, annular tears, vertebral endplate defects, disc space narrowing, and a worsening of degenerative disc disease in the study group as compared to the control group. [1] These results led Dr. Carragee to conclude, "...careful consideration of the risk and benefit should be used in recommending procedures involving disc injection." In plain English, that means you should only poke a needle into the disc if absolutely necessary, for there are consequences to these types of procedures.
Annular Tear Classification Systems
When it comes to diagnosing discogenic pain, provocative discography with fluoroscopic guidance is the proverbial gold standard. The Dallas Discogram Classification System was originally described in the late 1980s (126,118), but has since been modified twice. However, many examiners still use the original system; therefore, I believe it is useful describing it below in detail.
Dallas Discogram Classification System: The Original System
 In order to really classify the disruption of the disc, the patient must have undergone CT scan immediately following the discography procedure. In a nutshell, the further away from the nucleus the tear is, the higher the grade rating.
In order to really classify the disruption of the disc, the patient must have undergone CT scan immediately following the discography procedure. In a nutshell, the further away from the nucleus the tear is, the higher the grade rating.
Grade 0: this means that all of the die that was injected into the nucleus pulposus, remains within the nucleus pulposus. In other words, there is no tearing of the annulus fibrosus.
Grade 1: A small annular tear (black arrow, figure #1) is visualized extending from the nucleus into the inner region of the annulus fibrosis. Fig. #1 demonstrates what this might look like on axial CT imagery (although the needle that delivered the contract material into the center of the disc would be long-gone by this time).
Note the needle has injected a radio-opaque dye (pink) into the center of the disc (nucleus) which is used as a 'marker'.
At about 5 O' Clock (black arrow) a 'tear' or 'fissure' has become visible from the leakage of some contrast material. It extends from the nucleus radially into the inner 1/3 of the annulus fibrosus.
 This fissure or tear (the research community is trying to get away from the word "tear" which would indicate the lesion is always painful) would probably not be painful since there are usually no pain fibers in this region. This could be described as a 'Grade 1 Radial Annular Tear', or Grade 1 Internal Disc Disruption (IDD).
This fissure or tear (the research community is trying to get away from the word "tear" which would indicate the lesion is always painful) would probably not be painful since there are usually no pain fibers in this region. This could be described as a 'Grade 1 Radial Annular Tear', or Grade 1 Internal Disc Disruption (IDD).
Grade 2: (not shown here but you can see it on the discography chart below) now that the annular tear has grown larger in magnitude and is not only ripped its way through the inner one third of the annulus, but is now within the middle one third of the annulus.
This type of annular tear is still not believed to be painful because, again, the sinuvertebral nerves, which are the ones that carry the sensation of pain, are typically only in the outer one third of the annulus fibrosus.
Grade 3: the annular tear has now completely ripped through the annulus fibrosus. (figure #2) This type of tear is also called a "full thickness annular tear" or "radial annular tear."
The key to making this diagnosis, however, is that no contrast material is leaking out the back of the tear and no nucleus pulposus material has extended out the back of the tear. Therefore, the the posterior longitudinal ligament is still intact (blue) and is holding back the nucleus pulposus.
Can Grade 3 Annular Tear Be Painful?
I have devoted an entire page to these full thickness radial annular tears. But in short, yes! They absolutely can be painful in some, but not all patients.
 Grade 4: although there is no herniation of disc material yet, the tear is now spreading out concentrically to resemble a "ship anchor" on the overhead (axial) view. If you've studied the annular tear page, you will now know that this is the type of annular tear that often results in the high-intensity zone (HIZ) phenomenon that is visualized and T2 weighted MRI imaging in some patients.
Grade 4: although there is no herniation of disc material yet, the tear is now spreading out concentrically to resemble a "ship anchor" on the overhead (axial) view. If you've studied the annular tear page, you will now know that this is the type of annular tear that often results in the high-intensity zone (HIZ) phenomenon that is visualized and T2 weighted MRI imaging in some patients.
Anecdotally, these types of tears can be extremely painful because more sinuvertebral nerves are now exposed to nucleus pulposus. Therefore, there is a greater chance that a painful inflammatory process can occur.
figure #3 represents a grade 4 annular tear. Note the ship anchor appearance.
Grade 5: figure number three also represents a grade 5 annular tear because it's actually leaking! Therefore, a grade 5 annular tear simply means that the annular tear is leaking contrast material right out into the epidural space.
Therefore, a grade 3 and a grade 4 can both turn into a grade 5 annular tear simply by leaking contrast material out the back of the disc/annular tear.
Now we have a hole new dimension with regard to pain, because what is located posteriorly to the disc? The thecal sac, the traversing nerve roots, and the exiting nerve roots. So what? I don't get it? What happens if the nucleus pulposus and its degenerative chemicals (cytokines) soak into the nerve roots?
Anecdotally, it is possible that a inflammation process could start in these nerve roots which in turn sparks a true radicular pain (sciatica) and even radiculopathy (damaged reflexes and/or muscles in the lower extremities)!
Although anecdotally rare, I have come across patients with true radiculopathy secondary to a leaking annular tear. It is believed these patients are almost allergic to the cytokines and nucleus pulposus cells that leak out of the disc and soak into the nerve roots. The allergic response, of course is a form of inflammation and it kills axons within the nerve roots, which results in pain, decreased motor power, and/or decreased sensation and/or decreased reflexes.
Modern Discography:
The 'Modified Dallas Discogram Description' was finalized in the 1990's and is the 'Gold Standard' for the classification of annular tears. It was initially developed by a group of researchers from Texas (as described above in detail) (126), 'modified' by Bogduk et al. (7) in 1992, and then finally modified by Schellhas et al. in 1996(15). Below is a brief look at what that system looks like: (Sorry for getting off topic here!)
 The chart on the left demonstrates the five possible severities of the radial angular tear, as seen on an axial CT image. (In reality things are not always so 'nice and need' on discography but often they are.)
The chart on the left demonstrates the five possible severities of the radial angular tear, as seen on an axial CT image. (In reality things are not always so 'nice and need' on discography but often they are.)
The grade 0 is a normal disc, where no contrast material (red stuff that was injected into the center of the disc) has leaked from the confines of the nucleus.
The grade 1 tear has leaked contrast material but only into the inner 1/3 of the annulus.
The grade 2 tear has leaked contrast from the nucleus into the outer 2/3s of the annulus.
The grade 3 tear has leaked contrast completely through all three zones of the annulus. This tear is now believed to be painful since the outer 1/3 of the disc has many tiny nerve fibers that may now be irritated.
The grade 4 tear further describes the grade 3 tear, in that, now the contract has spread circumferentially around the disc, often resembling a ships anchor. To qualify as a grade 4 tear tear, the circumferential spread must be greater than 30 degrees. (Pathologically, this represents the merging of a full thickness radial tear with a concentric annular tear.)
The 'evil' grade 5 tear describes either a grade 3 or grade 4 radial tear that has completely ruptured that outer layers of disc and is 'leaking' contract material from the disc into the epidural space. This type of tear is thought to have the ability to induce a severe inflammatory reaction in 'some' peoples posterior neural structures. In some cases this inflammatory process is so severe is causes a painful 'chemical radiculopathy' and sciatica 'without' even the presents of nerve root compression.
References
1) Carragee EJ, et al. 2009 ISSLS Prize Winner: Does discography cause accelerated progression of degeneration changes in the lumbar disc. A 10-year matched cohort study. Spine 2009; 34:2338-45.
5) Osti OL, et al. Volvo Award - "Anulus Tears & Intervertebral Disc Degeneration: an Animal Model" - Spine 1990; 15(8):762-766
27) Moore RJ, et al. "Remodeling of Vertebral Bone after Outer Anular Injury in Sheep." – Spine 1996;21(8):936-940
28) Key JA, Ford LT "Experimental intervertebral disc lesions" – J Bone Joint Surg 30A:621, 1948
29) Moore RJ et al "Changes in Endplate Vascularity After an Outer Anulus Tear in the Sheep" – Spine 1992; 17(8):874-877
30) Kim KS, Yoon ST, Li J, Park JS, Hutton WC. 'Disc degeneration in the rabbit: a biochemical and radiological comparison between four disc injury model s. Spine. 2005 Jan 1;30(1):33-7.
118) Moneta GB, et al. "Reported pain during lumbar discography as a function of annular disruption and disc degeneration." Spine 1994; 19:1968-74
126) Sach BL, et al. " Dallas discogram description: A new classification of CT/discography in low back disorders. Spine 1987 ;12:287 -94