
PATHOLOGICAL DISC AGING: DEGENERATIVE DISC DISEASE
Structural Damage | Vicious Cycle of DDD | Genetics | Evil End-Phases | Disc Degeneration (pg.1) |
DEGENERATIVE DISC DISEASE: the fundamentals
 It seems that about 10% of us humans will develop chronic, life-long, back pain as a result of an accelerated form of natural disc aging, which is thought to be traumatically induced at least to some degree. This type of pathological disc aging is called Degenerative Disc Disease (DDD). It is important to keep in mind that many doctors incorrectly use the terms DDD and natural disc aging interchangeable.
It seems that about 10% of us humans will develop chronic, life-long, back pain as a result of an accelerated form of natural disc aging, which is thought to be traumatically induced at least to some degree. This type of pathological disc aging is called Degenerative Disc Disease (DDD). It is important to keep in mind that many doctors incorrectly use the terms DDD and natural disc aging interchangeable.
Fig. #1: Here we have a moderately to severely degenerated disc with 'structural disruption'. Note that dehydration and fibrous thickening is so great that we have lost much of the distinction between nucleus and anulus. If you look closely you can see evidence that the nucleus has lose 'hydrostatic pressure' and the inner lamellae are being sucked inward as a result (I've blackened one of the lamellae to help you see this inward buckling); this is an excellent example of DDD, probably as the result of structural damage to the upper and lower vertebral end-plate.
DDD includes all of the mechanisms of natural disc aging that we have discussed above but goes a step farther and includes often painful anular tears (216), disc protrusions (303) arrant nerve ingrowth (900), and stenosis.
There are two major risk factors that increase the chance of someone developing debilitating DDD: 1) Traumatically induced 'Structural Damage' to either the anulus fibrosus or the vertebral end-plate (12,59,16). 2) 'Inheritance and/or Poor Genetics', which research has demonstrated to be the single greatest risk-factor for DDD (505,411). Let's explore the major risk factors more in depth:
1) 'Structural Damage' to the Disc:
The 'Structural Damage Theory' (as I call it) of DDD, Championed by the legendary Bogduk and Adams (12,16,59), is based on the premise that any sudden loss of nuclear hydrostatic pressure (as a result of end-plate fracture/micro-fracture, and/or inner anular disruption) will result in a sudden and devastating 'axial-load-shift' (weight bearing shift) from the 'deflated' nucleus, onto the posterior anulus, ring apophysis, and zygapophyseal joints (12,59,16). Fig. #1 is a good example of this: in this disc, there was such poor pressure within the nucleus, the inner anulus (lamellae) were sucked inward, resulting in a 'inward buckling' (a tell-tale sign of DDD) phenomenon. This extra pressure upon the posterior anulus not only results in visible changes, but has also resulted in biochemical changes (MMP-3 secretion) that encourage the break down (degradation) and weakening of the anulus, hence encouraging the genesis of a painful anular tear (IDD) and/or which may disc herniation (19).
Fig. #2: A little refresher on how the disc carries the weight-load (axial-load) of the body. When the anulus is strong and the nucleus is well hydrated, there is an even distribution of load across the end-plate (12, 16) Note how the lamellae are bowed outward from the highly pressurized nucleus (pink zone). Just the opposite of Fig. #1, where the lamellae of the inner anulus were bowed inward.
Now let's take a look at what happens when something lets the air out of the 'beach-ball' and the nucleus looses hydrostatic pressure. End-plate and/or disruption of the inner anulus can both resulting in 'deflating' the nucleus and initiating DDD.
 Fig. #3: Here you can plainly see that the superior end-plate has buckled upward (like the real disc in Fig. #1) and allowed nuclear material to escape into and through the end-plate. This would be called a 'Schmorl's Node', and is responsible for 'letting the air out of our beach-ball', or increasing the volume within the nucleus, which in turn decreases hydrostatic pressure. (We discussed this vicious cycle of Disc Aging back on page 1, and will discuss the 'vicious cycle of degeneration below'). Note how the weight-load has markedly increase on the periphery of the disc, especially on the posterior of the disc and is absent in the center of the end-plate. We shall see the effects of this below, but they include: IDD, Disc herniation, Nerve in-growth, and stenosis.
Fig. #3: Here you can plainly see that the superior end-plate has buckled upward (like the real disc in Fig. #1) and allowed nuclear material to escape into and through the end-plate. This would be called a 'Schmorl's Node', and is responsible for 'letting the air out of our beach-ball', or increasing the volume within the nucleus, which in turn decreases hydrostatic pressure. (We discussed this vicious cycle of Disc Aging back on page 1, and will discuss the 'vicious cycle of degeneration below'). Note how the weight-load has markedly increase on the periphery of the disc, especially on the posterior of the disc and is absent in the center of the end-plate. We shall see the effects of this below, but they include: IDD, Disc herniation, Nerve in-growth, and stenosis.
The Vertebral End-Plate: The Achilles' Heal of the disc.
The vertebral end-plates are definitely the 'Achilles' Heal' of the motion segment (16) (two vertebrae and the disc in-between), and are easily damaged by 'axial over-load injuries'; such as a fall on the buttock, lifting something that is way too heavy, or from repetitively lifting something moderately heavy (fatigue failure) (16). It has been repeatedly demonstrated that when the motion segment is experimentally compressed to point of 'failure', it's almost always the end-plates that 'breaks' first, NOT disc (30-33).
It's also known that it doesn't take much end-plate damage to trigger this 'axial load-shift' which I illustrated above in figures #2 and #3. Adams et al. has experimentally determined that only "minor compressive damage to a middle-age vertebra" will result in a "large and progressive" axial load-shift, that always upon the posterior anulus (16).
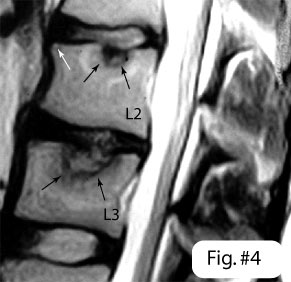 Fig. #4: Schmorl's Nodes (SNs): On this lateral T2-weighted MRI image, we have and example of two SNs, which are one of the most common type of end-plate disruptions. These typically occur in around 50% of the population, usually in the thoracolumbar junction (T12, T11, & L1) (34). Often, SNs are rather small in size but if they get big (as depicted in fig.#4), not only can they cause back pain, but they may also trigger the DDD process via a fatal loss of hydrostatic nuclear pressure (see more on this below). Note the disc below the L3 vertebra is white, healthy, and non-degenerated. The L3 disc (between L2 and L3) has been prematurely degenerated (black appearance) as the result of a huge traumatically induced Schmorl's Node (white arrows) which occurred as the result of a ski jumping accident. The L2 upper front corner of the vertebra has suffered an old compression fracture (white arrow) and another good sized SN is noted in the upper vertebral end-plate. The disc, although not as arid, has collapsed by about 50% (as has the L2/3 disc) which is classic of DDD.
Fig. #4: Schmorl's Nodes (SNs): On this lateral T2-weighted MRI image, we have and example of two SNs, which are one of the most common type of end-plate disruptions. These typically occur in around 50% of the population, usually in the thoracolumbar junction (T12, T11, & L1) (34). Often, SNs are rather small in size but if they get big (as depicted in fig.#4), not only can they cause back pain, but they may also trigger the DDD process via a fatal loss of hydrostatic nuclear pressure (see more on this below). Note the disc below the L3 vertebra is white, healthy, and non-degenerated. The L3 disc (between L2 and L3) has been prematurely degenerated (black appearance) as the result of a huge traumatically induced Schmorl's Node (white arrows) which occurred as the result of a ski jumping accident. The L2 upper front corner of the vertebra has suffered an old compression fracture (white arrow) and another good sized SN is noted in the upper vertebral end-plate. The disc, although not as arid, has collapsed by about 50% (as has the L2/3 disc) which is classic of DDD.
Abnormal Hydrostatic Pressure accelerates disc degeneration:
Both Handa et al. (11) as well as Ishihara (20) have concluded experimentally that disc cells are very picky about the amount of hydrostatic pressure that they can function in. They thrive at 3 atm of hydrostatic pressure, which just happens to be the normal pressure of a non-degenerated disc. Any variation in that pressure, EITHER higher (>30 atm) or especially lower (< 1 atm) will stop that disc from functioning (making proteoglycan which hold water within the disc). I described this 'vicious cycle of aging back on page #1.
When the vertebral end-plates or inner anulus become disrupted, as in fig. #4, the 'volume' of the nucleus is increased (the nucleus has gained extra space), which in turn causes an immediate and sudden drop in the hydrostatic pressure within that nucleus (23). In order to get that nuclear pressure back up, the disc cells would have to kick into 'over-drive' and make proteoglycan (which would suck up more water and resort hydrostatic pressure). Unfortunately, as noted in the above paragraph, the cells of the human the disc cells turn OFF in response to lowered hydrostatic pressure (< 1 atm) (11,20) instead of ON, so there is no chance to 'pump that nucleus back up'. To make matters even worse, since many disc cells are no longer making proteoglycan, the hydrostatic pressure falls even lower which turns off even more cells and a vicious cycle is born. This vicious cycle shifts more and more 'axial-load' onto the posterior anulus, hence worsening the degradation of the anulus even more.
2) Inheritance and Poor Genetic: The number 1 risk factor of DDD.
There are three areas of study in this sub-field of disc degeneration: Familial associations, unspecific genetic twin studies, and specific gene studies.
A) Familial Risk factors for DDD:
IF IT'S IN THE FAMILY WATCH OUT: There are two studies that strongly indicate that genes for DDD do exists and carry a significantly high risk factor for the passage of DDD and its evil end-phases (disc herniation in these studies) to the off-spring.
In 1998, Matsui L et al. (398) demonstrated for the first time that moderate to severe disc degeneration was strongly associated with a family history of past disc surgery. This study evaluated two groups of patients (gender and age matched) that were both suffering from lower back pain and/or unilateral leg pain. The "study group" consisted of first-degree family members from patients who had undergone disc surgery. The "control group" consisted of back pain patients who had no history of disc surgery amongst their first-degree family members. Both groups were suffering back and/or leg pain of equal duration and intensity. Next, all members of the study and control group underwent an MRI study to check for degenerative disc disease. RESULTS: The study group was twice as likely to demonstrate moderate and severe degenerative disc disease (DDD) in the critical lower lumbar discs than did the control group. Matsui concluded that paper by saying, "there may be a genetic factor and familial predisposition in the development of lumbar disc herniation as an expression of disc degeneration." (398) Other investigations have demonstrated this same finding. (396,397,399)
DISCOGENIC BACK PAIN & DISC SURGERY'S "FAMILY CONNECTION."
Having a first-degree family member who suffers discogenic back pain and/or who has undergone disc surgery also significantly increases the chances of another first-degree family member suffering the same fate: In 1998 Postacchini demonstrated that there is a strong familial predisposition to discogenic back pain and even disc surgery. The researchers studies the first-degree relatives (parents, siblings, and children) of three groups of people: Group 1 was comprised of 284 patients suffering discogenic back pain, Group 2 consisted of patients who had undergone lumbar disc surgery, and Group 3 consisted of 280 asymptomatic people who had never had back pain before. After questioning the first-degree relatives of each group, the researchers found that 37% of the surgery group had at least one member of the family suffering discogenic back pain as well and 10% of the surgery group had at least one member of the family who had also undergone disc surgery. On the other hand, only 12% and 1% of the first-degree relatives of the asymptomatic people suffered discogenic back pain and underwent disc surgery respectively. This clearly demonstrates that having a family history of spine surgery significantly increases the chances that another member of the immediate family will also suffer discogenic pain (3 times more likely), and even disc surgery (10 times more likely). Postacchini concluded this investigation by stating “this study indicates that there is a strong familial predisposition to discogenic low-back pain, and suggests that the etiology of degenerative disc disease is related to both genetic factors… and environmental factors.” (395)
So, if you have someone in your family who has crippling arthritis, or who has had back or neck surgery as the result of the end-phases of DDD, there is a chance that you may be at risk to suffer their fate as well.
B) Gene Mutations and DDD:
Even more striking than DDDs connection to familial factors, is that between certain gene mutations and DDD.
Based on a fairly recent, 'Volvo Award Winning' Twin study, 'inheritance' has been determined to be the largest single 'risk-factor' of a person developing DDD (403) and this inheritance is at least partly genetic in nature (413a). It now seem likely that there may well be 'genetic weaknesses' in the collagen framework of the disc and/or genetic influences on blood supply and disc metabolism (413a). There may also be 'genetic susceptibility' that may indirectly lead to DDD such as genetically small discs, a heavy torso, or small internal levers. The latter factors may all over-whelm the disc and lead to DDD.
Gene mutations occurring within the structural make-up of the disc have also been recently discovered. Here are some of these recent and exciting mutations:
Two mutations (polymorphisms) have been found within the genes that produce discal collagen (type IX collagen). These gene mutations have been named COL9A2 and COL9A3. Although the occurrence of this type of gene mutation is rare, when it does occur, the association with disc degeneration and sciatica are extremely strong (406,407, 408).
Another gene mutation has been associated with the discal proteoglycan aggrecan molecule (409, 410). You remember how important aggrecan molecules are right? Remember that they attract and hold water within the disc, which disc the disc high hydrostatic pressure. This particular devastating gene mutation produces a non-water absorbing aggrecan! Yikes! This gene ultimately results in severe disc dehydration and greatly increases the chance for IDD, and disc herniation (409, 410).
Recently, a mutation within the Vitamin D receptor gene has been associated with DD although the mechanism is still not clear (411a, 412, 413,414).
Other gene mutations have been strongly associated with disc bulging, anular tearing (IDD) and osteophytosis (412, 417).
I'm sure we will hear a lot more about this fascinating research area in the near future. In future there may a blood test that will warn you if your susceptible for the development of DDD and its 'evil end-phases'. This could help you chose a line of work that was conducive to the strength of you discs and maybe help prevent a middle aged catastrophe!
C. Other Risk Factors of DDD:
Occupation:
In 2000, Luoma et al. (201) conducted an excellent study on the relationship between DDD, pain, and occupation. They found that occupation type was strongly related to lower back pain and sciatica, however, DDD was only somewhat associate with these pains. Here's the study in a 'nut-shell':
A moderate sized (50 - 60) group of construction workers [heavy lifting], heavy equipment operators [vibration & prolonged sitting], and office workers [sit & stand light work] were followed for four years via questionnaire & nurse interview. At the end of the four years a MRI, interview, and final questionnaire was done on each participant. Results: Over the last year, and over the last four years the heavy equipment operators has about 50% more sciatica (nonspecific) than the construction workers, and 66% more sciatica than the office worker. The office workers did the best and had about 25 to 30% less back/leg pain over the four year period. Interesting, despite all this sciatica (over 50% of the heavy equipment operators had complained of leg pain) there were NO disc herniation found in any of the groups! So, lower back pain and leg pain does seem to be related to occupation. DDD (defined at disc bulging and a black nucleus on T2-weighted MRI) was also associated with back pain and sciatica not nearly as strongly as was occupation was.
Cigarette Smoking:
Cigarette smoking with a disc condition is just a bad idea! In 1991, Battie et al. (28) won the Volvo Award for her discovery that smoking increased spinal disc degeneration (across all discs!) by nearly 20%! She did this by using twin pairs that were discordant (one twin smoked with the other twin didn't) for smoking. I personally know several spinal surgeons who will NOT perform surgery unless the patient is 'smoke-free' for at least three months. It has been theorized that smoking damages the already compromised capillary beds (which reduces nutrient supply to the disc and dehydrates the disc) above the vertebral end-plates.
The 'Evil' End-Phases of DDD: Here's where the pain begins!
As I've mentioned back at the beginning of this paper, it's not the beginning phases of DDD that are painful. The pain begins when the intervertebral disc becomes disrupted and disorganized. Let's discuss some of the possible 'end-phases' of DDD:
#1) Internal Disc Disruption (IDD) and Disc Herniations:
 We have learned that the outer 1/3 of the intervertebral disc and perianular tissue are filled with tiny pain-sensitive nerve fiber (701-705). Because of the 'vicious cycle' of DDD (here) the nuclear clefts and fissures that are commonly produced as the result of natural disc aging, will begin to coalesce in to larger outward projecting structures called radial anular tears (aka: radial fissures, internal disc disruption or IDD). With time and continued axial trauma, these tears may completely bisect the disc, as depicted in Fig. #5, and allow 'caustic' nuclear material to course into the pain sensitive outer regions of the disc. This may well result in what we call 'discogenic' lower back pain. (For further information on anular tears, please see: concentric tears | rim lesions | radial tears )
We have learned that the outer 1/3 of the intervertebral disc and perianular tissue are filled with tiny pain-sensitive nerve fiber (701-705). Because of the 'vicious cycle' of DDD (here) the nuclear clefts and fissures that are commonly produced as the result of natural disc aging, will begin to coalesce in to larger outward projecting structures called radial anular tears (aka: radial fissures, internal disc disruption or IDD). With time and continued axial trauma, these tears may completely bisect the disc, as depicted in Fig. #5, and allow 'caustic' nuclear material to course into the pain sensitive outer regions of the disc. This may well result in what we call 'discogenic' lower back pain. (For further information on anular tears, please see: concentric tears | rim lesions | radial tears )
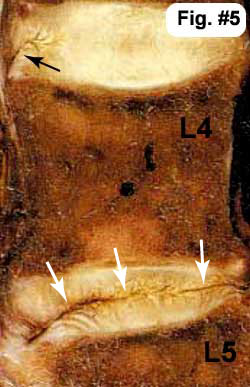
Fig. #5: Here, the L4 disc (between the L4 and L5 bones) is completely disrupted with a full thickness radial anular tear running from front to back. Its so obvious I didn't even label it, for the ugly dark line that appears to split the disc into two, speaks for its self. Note the L3 disc (above the L4 vertebra) look pretty good (white and hydrated) except for that 'most excellent' example of a anular 'rim lesion' (black arrow) which is seen in the anterior outer most anulus, extending obliquely upwards. (This may also be a combination of a rim lesion into a concentric tear - which is know to produce the HIZ).
Disc herniations are born when the final layers of the anulus rupture and allow nuclear material to either collect behind the posterior longitudinal ligament (PLL) (this would be called a 'contained herniation' or 'protrusion'), or extrude into the peridural space (this would be called an extrusion or non-contained herniation) and compress the sensitive posterior nerve roots, dura of the cauda equina, dorsal root ganglion (DRG), and/or spinal nerve root. Now, the patient may develop 'true' radicular pain (true sciatica) which is often worse than the lower back pain. These topics will be covered separately on another page.
#2) Nerve In-growth :
There is mounting evidence that a diseased disc (DDD) may be generating pain from deep within its own tissue (900,904,905,906)! For years it's been taught that the nucleus, inner and central anulus are completely avascular and aneural (have no blood or nerves), and that only the very outer layers of the posterior and anterolateral anulus contain nerve fiber (701-705). There is now strong evidence that pain carrying nerve fibers can grow inward, deep into the middle anulus and even nucleus in some cases! Not only has this neural in-growth been found within degenerated discs, but recently it has even been linked to discogenic back pain!
In 1997, Freemont et al. obtained the discs of 30 patients who had undergone surgery (fusion) for chronic discogenic back pain. All of these discs had tested positive for concordant pain prior to the surgery, indicating that the disc were most likely the cause of the patients back pain (discogenic pain). The extracted discs were then studied microscopically and compared with fresh cadaver discs of victims who had no prior history of back problems.
RESULTS: Amazingly, 77% of the discogram positive fusion patients were found to have nerve fiber in-growth all the way into the middle 1/3 of the anulus; versus only 6% of the normal 'control' discs. Not only did this ingrown nerve fiber look like 'pain fiber', but some of it was associated with 'Substance P' expression (which is a neural transmitter involved with pain transmission). This is fairly strong proof that discogenic pain is related to nerve in-growth, as well as full thickness anular tears.
So a new frontier is born, although admittedly there is still much work to be done in this area of study.
#3) Stenosis as a result of DDD:
Stenosis is the 'end-of-the-line' when it comes to DDD and is usually an end-phase that is seen in the elderly (1). It is caused by that axial-load shift from the nucleus onto the posterior elements of the disc that we discussed in depth above ( here ). This weight bearing shift places great load/stress/strain upon the outer structures of the disc, not only affecting the anulus but also affecting the facet joints, especially when/if the disc begins to thin (12, 13). Human bone, as in the facet joints, responds to mechanical stress by making more bone in the areas of highest stress. This bony thickening is called hypertrophy . Stress induced hypertrophy is a good thing, for it makes the bone stronger and less apt to break under any newly imposed stress. Unfortunately, the facet joints just happen to form the posterior boarder a bony tunnel called the intervertebral foramen (IVF), in which the delicate and sensitive spinal nerve roots reside. IF our 'over-stressed' facet joints just happen to hypertrophy (thicken) too much, and in the wrong direction ( anteriorly ), a narrowing of the already narrow IVF will occur. The sensitive spinal nerves will slowly be crushed by the thickening facet, which leads to back pain, leg pain, lower limb weakness, and intermittent claudication (pain in the legs after a period of walking). This syndrome of facet joint hypertrophy into the IVF is called 'Stenosis', (lateral stenosis to be exact) and is a major concern for the elderly, i.e., it's the number one disabling spinal disorder in people over 65 (1).
Bony thickening/hypertrophy may also occur within the posterior ring apophysis, and if severe, may compress the front portion of the spinal cord (cauda equina). This type of stenosis is called 'central stenosis', and can also cause pain, motor loss, and bowel & bladder dysfunction (cauda equina syndrome).
The future: Biological therapies to the rescue? NOT
Researchers are futilely working on all sorts of ways to rejuvenate the dying and damaged disc tissue via both biological based therapy and gene related therapy - based on tissue engineering (21 ,24,25,47 ). I'm not even going to discuss this work for it is NOT an answer to DDD. At best is will only buy some extra pain for the disc, for until the underlying cause of DDD is address, i.e., loss of nutrition at the end-plate, any implanted or modified tissue will meet the same fate as the original tissue. Doh!!
It's not just I who believes their work is in vain. Famed researcher, author and multi-timed Volvo Award Winner, Dr. Norbert Boos, also politely insinuates that this line of research is 'doomed for failure' and advices the researchers to focus their efforts on ways of "tackling the discal inflammatory reactions (which seem to be the real 'ignition switch' of back and leg pain) at a molecular level instead of attempting tissue repair." (6)
Reference Page | Top | DDD pg.# 1 | Home
© Copyright 2002 – 2005 by Dr. Douglas M. Gillard DC - All rights reserved