PIRFT | IDET
One of the most difficult spinal conditions to treat is that of a symptomatic annular tear which has resulted in back and/or leg pain. This type of problem, which results in discogenic back and/or leg pain, has been completely recalcitrant to modern medicine's attempts to treat it.
In the late 1990s and early 2000s, researchers invented IDET and PIRFT in hopes of finding an effective treatment for discogenic back and/or leg pain.
The bottom line of of the forthcoming randomized placebo-controlled trials (these are very powerful and accurate studies if done correctly) demonstrated that neither PIRFT or IDET works any better than placebo for helping patients with their back and/or leg pain.
Let's take a look at both of these studies a little more closely, because there are still pain management doctors touting their efficacy, when they really shouldn't be.
PIRFT
Percutaneous intradiscal radiofrequency thermocoagulation or PIRFT is considered a minimally invasive procedure for low back pain and discogenic sciatica.
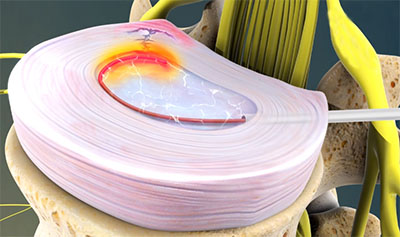
In a nutshell, the doctor carefully places a tiny cannula (like a straw) within the center of the disk that is thought to be pain generating. This is of course accomplished under fluoroscopic guidance. Then a wire or coil is placed in the very center of the disc. An RF generator is turned on which heats up the wire or coil to the point it starts destroying the disc from the inside out.
In reality, PIRFT it is very similar to the nucleoplasty procedure only the goals are different. Remember with nucleoplasty, you are trying to shrink their circumference of the disc which in turn reduces the size of a small contained herniation and therefore takes compression off a nerve root, reducing sciatica.
The theory is that by destroying the inside of the disc with thermal energy, it will reduce the number of cytokines (gasoline) which could leak into an annular tear and generate inflammation and pain. It is also believed that the heating will deaden the sinuvertebral nerves, which don't actually live in the center of the disc at all and normal people; however, in patients with chronic annular tears, sinuvertebral nerves can grow into the center of the disc.
The problem is, however, that the pain-generating region is most likely the periphery of the disc that surrounds the annular tear, and is heating is not going to affect that region. Therefore, it's not surprising this type of treatment failed.
Let's take a look at a 2009 randomized placebo-controlled trial, which focuses on PIRFT as a treatment intervention for low back pain.
Kvarstein G, et al. “A randomized double-blind controlled trial of intra-annular radiofrequency thermal disc therapy – a 12 month follow-up.” (2009) Pain Oct;145(3):279-86. Norway.
In 2009, Kvarstein et al published the results of rare, randomized double-blind controlled trial comparing the discTRODE probe (the procedure is called percutaneous intradiscal radiofrequency thermocoagulation [PIRFT]) against a sham treatment.
More specifically, 20 patients with chronic low back pain and one-level pressure-controlled provocation discopathy were randomized to either PIRFT or intra-annular sham treatment (placebo). At six months status post procedure, a blind assessment was performed on all 20 patients. The six-month analysis did not reveal any statistical trend to favor PIRFT over the sham treatment. That is, there was no difference in pain between the two groups. Because of this poor finding, no further patients were added to the study as planned.
After 12 months there was still no statistical difference between the groups, although "the outcome measures (ODI, SF 36 and VAS) appeared more promising (they were showing some improvement over the sham treatment but not enough to say for sure that it was working).
CONCLUSION
In conclusion, the researchers stated "the study did not finding evidence for a benefit of PIRFT, although a moderate effect cannot be ruled out. Considering the high number, reporting increased pain in our study, we would not recommend intra-annular thermal therapy with discTRODE probe."
IDET:
Intradiscal electrothermal therapy (IDET) was invented by a couple of pain management doctors in my neck of the woods-- the San Francisco Bay Area.
With this procedure, under fluoroscopy attempts are made to guide the tip of the wire as close to the annular tear as possible. Then, once again RF energy is applied to the tip of that wire and the doctor tries to burn shut the annular tear and kill off any pain-generating nerves in the vicinity.
The obvious problem with this treatment is wire tip placement. Annular tears can be through the full height of the disc or could be made of various heights. So it would be impossible to cover the entire tear in most cases. Another problem is the fact the doctor cannot see the annular tear at all under fluoroscopy; therefore, he or she is flying completely blind with regard to placing that needle tip.
Therefore, it was no surprise that the forthcoming randomized double-blind controlled trial failed to demonstrate that IDET was an effective for the treatment of discogenic pain or any type of back pain for that matter.
Freeman BJ, Fraser RD, et al. “A randomized, double-blind, controlled trial: intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain." (2005) Nov 1;30(21):2368-77; discussion 2378.
In 2005, Freeman et al published the results of another rare randomized, double-blind, controlled trial that randomly placed 57 chronic low back pain patients in either a intradiscal electrothermal (IDET) group or a sham procedure (placebo). (The respective ratio was 2:1). All of the patients had either one-or two-level symptomatic disc degeneration with posterior or posterolateral annular tears (as determined by provocative computerized tomography discography). The surgeon, patient, and independent outcome assessor were all blinded to the treatment.
Before the patients underwent the procedure, a battery of outcome evaluation tools were administered. These included the short form 36 questionnaire [SF-36], Oswestry disability index [ODI], Zung Depression Index, Low Back Outcome Score, and the Modified Somatic Perceptions Questionnaire).
RESULTS:
At the six-month time point, not a single outcome tool showed evidence that patients from either group had demonstrated any statistically significant signs of improvement. For example, the ODI for the IDET procedure was 41.2 at baseline and 39.77 at the six-month time point. For the placebo group, the ODI was 40.74 at baseline and 41.58 at the six-month time point.
CONCLUSION
In conclusion, the authors stated, "No subject in either arm [IDET or placebo] met criteria for successful outcome. This study demonstrates no significant benefit from IDET over placebo."