Introduction | Material & Methods | Five-Year Accessment | Discussion | Conclusion
Yao N, et al. “Full-endoscopic technique for anterior cervical discectomy and interbody fusion: a five-year follow-up results of 67 cases.” Eur Spine J. 2011; 20(6):899-904. Epub 2010 Dec 11. People's Republic of China.
In 2011, the research team of Yao, Wang, Wang and Wang published a one-of-a kind investigation into the efficacy (effectiveness) of anterior cervical discectomy and fusion (ACDF) performed through a 2 cm portal with a high-resolution endoscope. In addition to the fact a study of this type had never been performed, the investigators were able to recall for follow-up examination an impressive 88% of the original cohort (patients) five years or more from the date of surgery.
INTRODUCTION
It has long been known that symptomatic cervical disc disease, i.e., disc herniations with or without compressive/irritative spondylosis, can cause patient pain and suffering, as well as significant neurologic morbidity – a phenomenon we call myelopathy [1, 2].
The standard of surgical care for such conditions is ACDF, which is traditionally performed as an open procedure and involves removing the diseased intervertebral disc and replacing it with a titanium cage and autograft bony implantation. Previous investigations have demonstrated this procedure to be safe, efficacious, and result in high patient satisfaction [3, 4, 5]. However, the procedure is not without its complications. More specifically, patients can suffer dysphagia, hematoma, recurrent laryngeal nerve palsy and even esophageal perforation [6].
In 1998, Fontanella described an endoscopic microsurgical technique for the treatment of herniated cervical discs that touted positive clinical outcomes [7]. More specifically, this Italian doctor performed endoscopic microsurgical techniques on 171 patients that "should have undergone traditional surgery….” At the one-year time point, he reported a 97% success rate with no incidents or major complications. He concluded by saying, “…The endoscopic microsurgical technique is an extremely advantageous and safe method." Of course there were many shortcomings to this pioneering investigation, including lack of randomization and a control.
In hopes of mitigating the affirmation potential complications with open ACDF, these researchers investigated utilizing an endoscopic approach to the procedure instead of the open approach.
MATERIALS AND METHODS
Between January 2000 and January 2004, 76 patients with confirmed symptomatic single-level cervical disc herniation were treated with ACDF performed endoscopically. Patient inclusion into the study was limited to those of whom suffered single-level cervical disc disease (i.e., disc herniation with or without spondylosis) with associated cervical spine pain, radiculopathy, myelopathy, or radiculomyelopathy. The mean age of this cohort was 50.3 years, which consisted slightly more of males than females. Patients with severe spondylosis and disc height loss were excluded from the study. Unfortunately, there was no open ACDF control group; therefore, blinded randomization could not occur.
All 76 patients underwent ACDF through a 2 cm portal (this is quite large). The size of the portal was sufficient to introduce and in plant the titanium cage and autograft material. There were no complications.
After a short rehabilitation period, all patients were accessed for pain and functional status. More specifically, their neck and arm pain was accessed with the classic visual analog scale (VAS). Their functional status was accessed by way of the Japanese Orthopedic Association Scoring System (JOA). Postoperative radiographs were also taken in order to document anterior disc space height.
Over the next several years the cohort was followed, and at the five-year time point, 88% of those patients were available for re-evaluation (that is a most excellent number for this far out). Nine patients lost at follow-up and were left out of the study and statistical calculations (that was a no no).
THE FIVE-YEAR ASSESSMENT: The Results
With regard to neck pain (accessed via VAS), the patients improved on average 66.2% at the five-year time point. Their arm pain fared even better as it improved by 76.2%. With regard to functional improvement (processed via JOA), the patients improved significantly less – 38.2%.
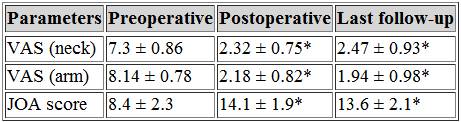
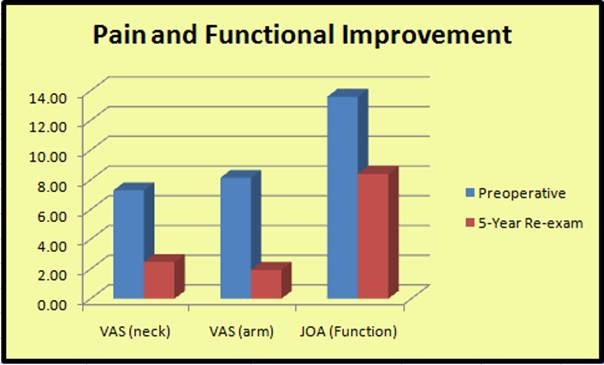
*Note: the JOA scores were inverted in order to create a better visual effect of improvement.
Other five-year outcomes included a 91.1% bony fusion rate at the five-year time point. Also noteworthy was the fact that there was a "slightly decreased" disc height at the five-year time point when compared to immediately following surgery.
DISCUSSION
This very long-term prospective outcome study successfully demonstrated that the time-tested, gold standard anterior cervical discectomy fusion (ACDF) could in fact be successfully completed through an endoscope with the use of a 2 cm portal.
In light of these results, the authors offered advantages of endoscopic ACDF that include rapid patient recovery, reduce surgical costs, diminished intraoperative soft tissue trauma, and less outcome morbidity.
The procedure, however, was not without concerns: the authors noted that there was a "steep learning curve" for the procedure, and they warned about limitations (due to limited workspace) with regard to major intraoperative bleeding. In the latter regard, they stated, “When the hemorrhage is unmanageable, a conversion to an open surgery is required immediately." They also stated that no traction devices could be used through the endoscope, which in turn eliminated this procedure for patients with severe spondylosis and discopathy (i.e., disc height loss).
CONCLUSION
Based upon the success of endoscopic ACDF, the researchers concluded, "Endoscopic ACDF with a 2 cm port appears to be a safe and potentially advantageous augmentation to this already successful procedure."
In closing, however, they acknowledged the need for a randomized blinded controlled trial in order to compare endoscopic versus traditional ACDF to substantiate their claims. No conflicts of interest were claimed.
REFERENCES
1) Ghogawala Z, et al. "Ventral versus dorsal decompression for cervical spondylotic myelopathy." Spine (2007) 32:429-436.
2) Rao RD, et al. "Operative treatment for cervical spondylotic myelopathy." J Bone Joint Surg AM (2006) 88:1619--1640.
3) Kambin P, Schaffer J. "percutaneous lumbar discectomy." (1998) Clin Orthop 234:24-34.
4) Raj DR et al. "Operative treatment for cervical spondylotic myelopathy." (2006) J Bone Joint Surg AM 88:1619-1640.
5) Silber JS et al. "Donor site morbidity after anterior iliac crest bone harvest for single-level anterior cervical discectomy infusion." (2003) Spine 28:134-139
6) Ono K, et al. "Myelopathy hand. New clinical signs of cervical cord damage." (1987) J Bone Joint Surg Br 69:215-219.
7) Dowd GC, Wirth FP. "Anterior cervical discectomy; this fusion necessary? (1999) J Neurosurg 90(Suppl 1): 8-12.