Introduction | The Study | The SED Procedure | Evaluation Method | Results | Discussion | Concerns & Comments
Tsou PM, Yeung CA, Yeung AT. "Posterolateral transforaminal selective endoscopic discectomy and thermal annuloplasty for chronic lumbar discogenic pain: a minimal access visualized intradiscal surgical procedure." Spine J. 2004; 4(5):564-573
Low back pain, which is known to effect about 70% all people at some point in their lives (711-712), is now recognized as the most common and costly ailment of the middle aged population in the western world (421). Luckily, most people will recover from this pain within one year; however, for an unlucky 5% of them, the pain will never completely resolve (342). That adds up to approximately 32 million people who suffer this type of chronic back pain in Europe and the United States alone!
It has been estimated that in 40% of these patients who suffer chronic back pain, the cause stems from disruptions or tears within the substance of the disc. And these tears somehow become sensitized and painful (10). The latter relatively common phenomenon, which has been termed Internal Disc Disruption (aka: IDD, or discogenic pain syndrome) (9), is the nemesis of patient and doctor alike, for it is very difficult to conservatively treat and often results in great patient suffering. Unfortunately, the only current mainstream treatment is the dreaded fusion surgery which empirically works in only one third of the patients.
As an alternative to traditional fusion, which carries an unacceptably high morbidity rate, the research community has been experimenting with new forms of treatment for Chronic Lumbar Discogenic Pain (CLDP). IDET, SED, Intradiscal Injection, and various forms of laser and RF annuloplasty are some of the new arrivals, although the efficacy of such procedures are yet to be fully demonstrated. (Note: the IDET procedure, which has the greatest body of research to date, has an investigation in-process that was randomized and double blinded; it is nearing the one year outcome mark and, if the 6 month results hold true, the study should confirm IDET is fairly effective for the treatment of IDD, and is far less costly and invasive than fusion. (11) [that study never panned out – IDET was not efficacious.]
In the the mid 1990s, Dr. Anthony Yeung, who specializes in endoscopic disc surgery, developed a treatment for CLDP. Officially, his procedure is called Selective Endoscopic Discectomy with Thermal Annuloplasty; however, more recently the acronym SED has replaced it longer birth name.
I like to describe SED as an eye-ball-guided debridement and cauterization of a damaged disc(s). More explicitly, the doctor will enter the torn disc with an endoscope--a device that allows the doctor to physically see inside the disc. After a workspace is carved out (that's kind of the scary part), a special dye (indigo carmine) is injected which stains the disc's degenerative areas. Then a visually hunt begins in which the doctor looks for and remove pieces of degenerated nucleus pulposus that may have broken off and migrated away from their home in the center of the disc (you could call these fragments the fledgling disc herniation). It is believed that fragments of nucleus pulposus that have wandered into this pain sensitive outer one third of the disc is at least in part the cause of IDD.
After the removal of these nuclear fragments, the doctor will proceed to burn (ablate) the annular tears (these annular tears may be considered channels that allow the nuclear material to escape to the periphery) in attempts to permanently close them. This appellation is done with a instrument called a radio-frequency (RF) probe (Ellman Trigger-flex RF probe). Besides physically sealing/closing the annular tear, it is hoped that this application process will destroy any pain sensitive nerve fiber that may have grown down into the annular tear. (904-906).
This 'pilot-like' (first of it's kind) investigation is thought to be the first in a series of studies focusing on the efficacy of SED as a treatment intervention for patients of whom suffer chronic low back pain secondary to IDD. Unfortunately, the study design was a simple retrospective type study and did not use randomization and/or placebo control.
Between January 1997 and December 1999, the senior author (Dr. Anthony Yeung) performed 151 SED procedures on patients with confirmed (via modified provocative discography) Chronic Lumbar Discogenic Pain (CLDP). There were 38 patients who needed SED performed at more than two levels–these two level patients were removed from the study, which left a total of 113 patients for this investigation.
All patient outcomes were retrospectively (reviewed long after the surgery) assessed by Dr. Paul Tsou, who was a fellow of Dr. Young.
That average age of the cohort (study group) was, as usual, about 41 years and the average back pain suffering-time was about 2 ½ years (minimum of 6 months); in other words, all of these patients failed at least 6 months worth of conservative care (exercise, activity modification, medication, and bracing) before succumbing to SED surgery.
As an important side note, the approximate pre-surgical disability level, as measured by the Oswestry Disability Index for this similar cohort, was 59, which denotes a "severe" functional impairment. In other words, this was a very symptomatic group of patients folks! (99)
Study Entry Criteria:
A modified form of the classic provocation discography (Evocative-chromo-discography) was wisely used as the corner stone for patient acceptance into this investigation (39). In other words, in order to gain entry into this investigation, the patients had to exhibit a strong degree of concordant pain (their usual & typical pain) upon discal pressurization. They also had to have a negative control disc (that is,pressurization of an adjacent disc did not cause any pain to the patient – only the bad/suspect disc was pain sensitive).
Other entry criteria included the following: a patient chief complaint of axial lower back pain with minimal or no associated lower limb painmust be present; the pain syndrome had to be present for at least 6 months (the average pain duration was 2 ½ years); the patient could have no more than two levels of discal involvement; and any anular bulges must not be greater than 5mm in size (as measured from the posterior vertebral margin). Generously, even severely degenerated discs that included loss of disc height were allowed into the investigation. Even more surprising still was the fact that some failed IDET cases were even allowed to participate (99)! (The doctors were not "cherry picking" in this study!)
 I’m going to keep this simple and recommend that for those of you who want to know more, please purchase the investigation – it’s available through www.pubmed.com. The investigators do an excellent job at describing the procedure and include some very well done illustrations.
I’m going to keep this simple and recommend that for those of you who want to know more, please purchase the investigation – it’s available through www.pubmed.com. The investigators do an excellent job at describing the procedure and include some very well done illustrations.
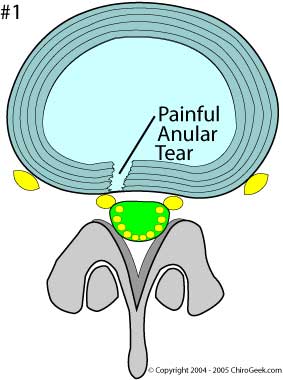
Figure #1 demonstrates Internal Disc Disruption (IDD):
If you need a review of the disc anatomy go here.
Note that the annulus (dark blue) of the disc has been torn through (disrupted) and has allowed degenerated nuclear material (light blue) to seep into that highly innervated (i.e., filled with tiny pain sensitive nerves – not shown) posterior 1/3 of the disc. (There may also be small fragments (chunks) of nuclear material in that tear as well - not shown in this example.) It's this seepage of degenerated nuclear material that is believed to be the major cause of discogenic pain.
Why is IDD so painful? It is theorized that in an attempt to heal the torn annulus, tiny blood vessels, as well as evil pain carrying nerve fibers will grow into the anular tear and/or vertebral end-plate (904-906). These newly formed blood vessels and nerve fibers are now 'exposed' to the irritating biochemicals (such as tumor necrosis factor alpha) of the nucleus, which in turn may cause an inflammatory pain syndrome, which in turn leads to the genesis of discogenic pain. To learn more about IDD go here.
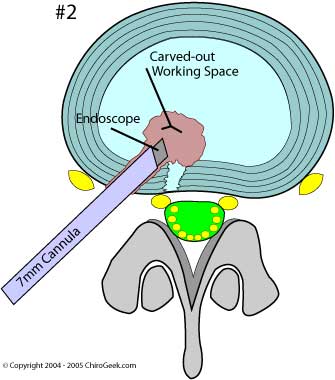
Figure #2 Depicts the SED procedure:
Here, in an attempt to de-nerve and heal the annular tear, we have surgically inserted a hollow cannula (light gray tube) into the back-lateral side of the disc and then carved out a "working space" within the annulus and nuclear region of the disc. (This punching a hole through the un-injured portion of the disc is the major concern within the procedure.""
The annulus and working space were created - or dug out - with a "two channel obturator" and a "rongeur / motorized shaver".
The endoscope (dark gray) allows the doctor to actually see what is going on within the disc and acts as the doctors eyes. A special stain (indigo carmine dye), which was initially injected into the disc before all the digging occurred, will assist the doctor in identifying the 'evil' degenerated nuclear material and is unique to this procedure. This visual verification of the pathological tissue and annular tear is what makes SED a much more scientifically sound procedure than attempts at treating IDD – such as IDET, which uses a two dimensional blind procedure.
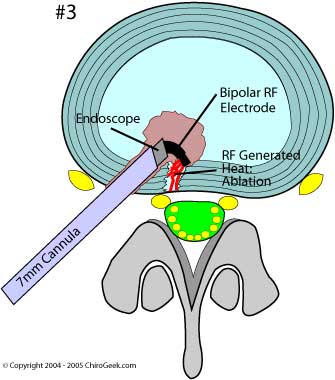
Figure #3 Depicts the Radio Frequency Ablation portion of the procedure:
The Bipolar RF Electrode has been inserted through the cannula and into the working space.
The doctor can now begin the hunt for any 'blue-stained' nuclear material that has gone astray and entered the anular tear. Once the doctor finds his target, i.e., degenerated disc material, it will be 'zapped' with the RF electrode and destroyed. This part of the procedure is called Ablation.
After all of the nuclear material is removed, both in and around the annular tear, the doctor's next task will be to attempt to seal/shrink that anular tear with the heat energy from the RF electrode. Sometimes laser is used for those hard-to-get-at annular tears.
The ablation of the annular tear will, theoretically, deaden the patient's pain by destroying any pain-generating nerve fiber that has grown down the annular tear.
THE EVALUATION METHOD: The Modified MacNab Criteria & The Patient Outcome Questionnaire
As with this group of researchers’ last investigation, two outcome assessment tools were chosen for use: the Modified MacNab criteria, and an unnamed patient questionnaire that was developed by Dr. Tsou. Although there were some modifications made to this questionnaire since last time, the investigators still failed to utilize any of the standard, time-test, ‘outcome assessment tools’, such as the Oswestry Disability Index, the Roland-Morris, or the Visual Analog Scale (VAS). (according to Dr. Young, this early over site has been corrected for and will be utilized in their next investigation).
The MacNab Criteria:
Each patient’s clinical data, which included chart notes; MRI images; discography results; surgery noted & video; and any follow-up assessment notes, were reviewed independently by doctor Tsou. The patient outcome results were graded as either excellent, good, fair, or poor based on the MacNab criteria (51) and a modification: if the patient answered yes or true to any of the following questions, an automatic ‘poor’ results was assigned: 1) Since my arthroscopic back surgery, my back/leg pain is no better or worse than before surgery; 2) I had a reoperation at the arthroscopic back surgery level; 3) My arthroscopic back surgery was not satisfactory; and 4) I will not select arthroscopic back surgery again if I encounter similar back problems in the future. IF none of the latter four statements applied to the patient, than the patients were placed into one of the following categories based on the MacNab Criteria: 1) No pain and no functional restrictions = Excellent Rating; 2) Occasional back/leg pain, brief functional restrictions = Good Rating; and 3) Improved overall function, permanent work and activities of daily living modification = Fair. (poor was not defined)
The Patient Questionnaire:
The patient-based questionnaire, which was mailed to the patients two or more years after their SED procedure was completed, required the patients to answer 8 relatively straight-forward questions regarding their over-all experience with the SED procedure. After completion, the questionnaire was mailed back to the researchers for review and tabulation. Here's the exact questionnaire: (For questions 1 through 4, simply choose the best answer.)
QUESTIONS: |
ANSWERS: |
| 1) After my arthroscopic back surgery, I returned to my usual occupation in: | a) 1-2 months; b) 3-6 months; c) 7-12 months; d) over 12 months. [dg--> where's never?] |
| 2) After my arthroscopic back surgery, I returned to my usual activities of daily living and recreation sports in: | a) 1-2 months; b) 3-6 months; c) 7-12 months; d) over 12 months. |
| 3) After my arthroscopic back surgery, I ceased to take prescription drugs in: | a) 1-2 months; b) 3-6 months; c) 7-12 months; d) over 12 months. |
| 4) My overall residual back/leg pain is: | a) None; b) mild, minimal functional adjustment; c) occasional, moderate work and activities of daily living modification; d) “was left out of paper!” |
| For the next questions, Mark 'TRUE' ONLY if statement applies to you: (note: if any one of the following was marked, the patient was automatically placed into the failed category.) | |
| 5) Since my arthroscopic back surgery, my back/leg pain is no better or worse than before surgery. | TRUE |
| 6) I had a reoperation at the arthroscopic back surgery level. | TRUE |
| 7) My arthroscopic back surgery was not satisfactory. | TRUE |
| 8) I will not select arthroscopic back surgery again if I encounter similar back problems in the future. | TRUE |
[Scoring: Question 1 through 3 are worth the following points: a) = 3 points; b) = 2 points; c) = 1 points; d) = 0 points. In question #4, the following points were awarded: complete=3 points; almost complete = 2 points; partial = 1 point; and no improvement = 0 points.]
Assuming that none of the last four questions (#5 - #8) were answered (which would have defaulted the patient into a ‘poor’ rating), the over-all patient SED outcome was made by simply adding up the points-awarded for question 1 – 4. Once you have this number, simply plug it into the following rating scale to see how the patient fared: 9 to 12 points = Excellent outcome; 5 to 8 points = Good outcome; 3 to 4 points = Fair outcome; 0 to 2 points = Poor.
SED Results at 2 year status-post |
MacNab Criteria (113/113 pats) 100% |
One Level SED Result (47/113 pats) |
Two Level SED Results (66/113 pats) |
Patient Questionnaire Results |
Excellent |
17 (15%) |
8 (17%) |
9 (13.6%) |
14 (16.9%) |
Good |
32 (28.3%) |
14 (29.8%) |
18 (27.3%) |
24 (28.9%) |
Fair |
34 (30.1%) |
13 (27.7%) |
21 (31.8%) |
26 (31.3%) |
Poor |
30 (26.5%) |
12 (25.5%) |
18 (27.3%) |
19 (22.9%) |
| Excellent, Good,& Fair | 83 (73.5%) |
64 (77.1%) |
||
Good & Excellent |
49 (43.3%) |
|
|
38 (45.8%) |
Patients that were satisfied enough to claim that they would have SED again: |
83 (73.5%) |
|
|
64 (77.1%) |
ASSESSMENT: My Two Cent's Worth:
The most impressive result of this investigation is the fact that about 75% of the patients, which contained a subgroup of 43 (39%) workers' compensation and personal injury patients (these type of patients are notorious for not reporting improvement secondary to ulterior motives– i.e., they are confounders), obtained at least some improvement from the SED procedure and would choose to have the procedure again given similar circumstances.
Anecdotally, their Oswestry scores fell from 59 (severely disabled) to about 23 (lower range of the moderate category); this is about a 39% drop (99). There was no information available on medication use or work status.
The fact that only about 45% of the patients obtained a good to excellent result was still a little disheartening for me; however, it must be remembered that this group of patients was not 'hand-picked' for success but represented a true group of severely disabled and suffering patients. In my conversation with Dr. Yeung, he mentioned that if he were to 'hand-pick' a group a perfect SED candidates, he could get "95%" of them in the good and excellent categories! (99)
The complication rate surrounding the SED procedure was quite low: three patients developed cases of dysesthesia (leg pains {I wonder what the mechanism of that would be?}) and one patient developed a case of thrombophlebitis. This 3.5% complication rate is certain quite acceptable and indicates that SED seems to be quite a safe procedure.
I’ve been waiting and waiting for this investigation to be made public, for SED is certainly a major ‘Buzz – word’ within the chronic pain internet community and has been haled by some as a “miraculous” and “revolutionary” means of treating discogenic back pain (26). Initially, I was quite disappointed by both the investigation design and the outcome results; however, when I e-mailed the senior author, and expressed my disappointment, he graciously began a series of e-mails that have certainly quelled my concerns to the point I have revised this page.
This investigation, which probably should have been called a 'pilot', was not intended to be a major scientific paper, but merely the first in a series of investigations into the efficacy of the SED procedure. I have been informed that the follow-up investigation will use better scientific outcome tools (Oswestry disability index), so a more comparative result may be yielded.
In my conversations with Dr. Yeung, he wanted it to be known that this investigation was geared toward the doctors in the "trenches" (i.e., clinical doctors who treat chronic low back pain and would consider using/ordering a SED procedure). He wanted to give them a real world study (hence the inclusion of the workers compensation / personal injury patients) and not a study where patients were hand-picked for success. In that regard, he stated that if he were to mirror the patient entry criteria of some of the recent investigations into IDET and Fusion, his SED procedure would have "better results than IDET and less morbidity than fusion." More explicitly, he stated that 85% to 95% of SED patients (using the stricter entry criteria) could expect a 'Good or Excellent' outcome result that should hold at least for two years after the surgery. (99)
So, in order to make this study a real 'in-the-trenchs' type investigation, the doctor did not greatly restrict the entry criteria and accepted some conditions that would have never been allow into other investigations, i.e., failed IDET patients; multi-level procedure patients (60% of cohort); patients with collapsed discs; and patients who were involved in litigation (39% of cohort). The meer fact that the average pre-SED Oswestry score (anecdotally calculated) was 59, demonstrates that these patients were going to be a tough bunch to treat and for some, SED was their last hope to avoid the dreaded fusion.
With the aforementioned in mind, its is quite impressive that 75% of this group of patients obtained at least a 'Fair' outcome at two years post SED and would elect to repeat the SED procedure if a similar pain syndrome developed in the future. The average Oswestry score(anecdotally calculated) plummeted 39% which, although didn't completely cure the patients from neither pain nor disability, at least gave the patients back some form of a life.
The ironic thing about the SED procedure - as I have already mentioned in my review of Dr. Yeung's Endoscopic Disc Herniation Excision procedure - is that in order to fix a painful annular tear within the disc, the procedure demands the creation of a new, man-made, annular tear! more specifically, the man-made annular tear results from punching the endoscope into the already irritated disk and then carving out a workspace.
So what, you might ask? We have a pretty good idea from animal research (100-105) that any puncturing of the outer annulus will not only lead to the progressive development of a full thickness anular tear, but also lead to a perpetuating degeneration within that disc. So it would seem logical that the 7mm hole created by this endoscopic procedure (here) may well be opening another can of worms for the already sensitized disc--it is probably dooming that disc to another annular tear and severe degeneration.
Worth the Risk? In this cohort, all of whom suffered severe disability secondary to discogenic back pain, the risk was undoubtably worth it. Since the alternatives to SED (i.e., interbody fusion) are so awful, I would also gamble on this procedure if my disability was that I.
On the other hand, I'm not sure that a discogenic pain patient with only a moderate disability (i.e.,Oswestry in the 20s) would be a good candidate for SED, as they probably would not benefit in the long-run from the creation of another, iatrogenic, annular tear within the already disrupted and sensitized disc. To my understanding, Dr. Yeung would not accept such a moderately disabled patient in the first place.
Dr. Yeung also told me that SED, like other minimally invasive surgery, is not designed to last a life time and tells his patients that they can expect an 85% relief from their back pain for two years or more; however, some may require a repeat procedure(s) if their pain worsens. On average, the doctor stated, SED seems to last about 5 years - as empirically noted by the fact that his clinic typically starts getting calls from patients who had previously undergone SED and now have increased pain. (99)
The final concern, unless you are extremely wealthy, is the cost of the procedure. From my understanding (26) the SED procedure costs in the neighborhood of $25,000.00, which certainly is in the ball park with other procedures (my microdiscectomy was over $35,000.00); however, since the procedure is performed on an in-patient basis, some insurance companies are not picking up this portion of the bill. In fairness, I also know that patients undergoing IDET, nucleoplasty, Intradiscal injections, and other RF annuloplasty procedures are enduring the same hardships as well: Just something food for thought.
In closing I would like to thank Dr. Yeung for taking the time out of his incredibly busy schedule to correspond with me regarding the SED procedure and the creation of this investigation. His candor regarding the long-term complications of the procedure was a breath of fresh air and he truly seems like a one-of-a-kind doctor.
I strongly believe that his innovate approaches for the treatment of spinal disorders will etch him into the medical history books as one of this country's greatest spinal endoscopic pioneers. There is no doubt in my mind that with the inevitable advancement of technology, his endoscopic procedures with become even less invasive, more effective.
I eagerly await Dr. Yeung's next SED investigation and hope that he will employ a slightly more standardized patient-selection protocol, as well as a better designed method of reporting the patient outcomes (Oswestry & VAS). I also pray that he will extend the follow-up of this investigation, so we may learn the long-term outcome of patients who undergo SED.
Of course a perfect investigation would be to randomize a group of IDD patients into a fusion group, a SED group and a do-nothing group (hell, why not throw a chiropractic group in there as well) and see how that all pans out! that would be the study of the century, but will ever happen--at least in my lifetime.
REFERENCES:
2) Yeung AT, Tsou PM. “Posterolateral Endoscopic Excision for Lumbar Disc Herniation.” Spine 2002; 27(7):722-731
9) Crock HV. “Internal disc disruption: A challenge to disc prolapse fifty years on.” Spine 1986 ;11(6):650-3
10) Schwarzer AC, Aprill CN, Derby R, Bogduk N, Kine G. “The prevalence and clinical features of Internal Disc Disruption in patients with Chronic Low Back Pain.” Spine 1995; 20(17):1878-1883
11) Pauza KJ, Bogduk N, et al. “A randomized, placebo-controlled trial of Intradiscal Electrothermal Therapy for the treatment of discogenic low back pain.” Spine J. 2004 Jan-Feb ;4(1):27-35
12) Abramovitz JN, Neff SR. Lumbar disc surgery: Results of the Prospective Lumbar Discectomy Study of the Joint Section of Disorders of the Spine and Peripheral Nerves of the American Association of Neurological Surgeons and the Congress of Neurological Surgeons.” Neurosurgery 1991; 29:301-8
26) Numerous personal e-mails to my ChiroGeek.com e-mail address from apparently successful SED recipients.
29) Taylor V, Deyo R, et al. “Patient-oriented outcome from low back surgery.” Spine 2000; 25:2445-52
39) Derby R, et al. “The ability of pressure-controlled discography to predict surgical and nonsurgical outcome.” Spine 1999; 24:364-71.
51) MacNab I. “negative disc exploration: an analysis of the cause of nerve root involvement in sixty-eight patients.” J Bone Joint Surg (Am) 1971 ;53:891-903
52) Henrik Weber , '1982 Volvo Award in Clinical Science' "Lumbar Disc Herniation: A controlled, Prospective Study with Ten Years of Observation." Spine - 1983; 8(2):131-140
99) Yeung AT. Personal E-mail communications 12-23-04;12-24-04.
100) Osti OL, et al. Volvo Award - "Anulus Tears & Intervertebral Disc Degeneration: an Animal Model" - Spine 1990; 15(8):762-766
102) Moore RJ, et al. “Remodeling of Vertebral Bone after Outer Anular Injury in Sheep.” – Spine 1996; 21(8):936-940
103) Moore RJ, Osti OL, Vernon -Roberts B, “Osteoarthrosis of the Facet Joints Resulting From Anular Rim Lesions” – Spine 1999; 24(6):519-524
104) Key JA, Ford LT “Experimental intervertebral disc lesions” – J Bone Joint Surg 30A:621, 1948
105) Moore RJ et al “Changes in Endplate Vascularity After an Outer Anulus Tear in the Sheep” – Spine 1992; 17(8):874-877
342) Frymoyer JW et al. “Risk factors in low back pain.” J Bone Joint Surg Am 1983; 65:213-218
421) Nachemson AL. Newest knowledge of low back pain (editorial comments). Clin Orthop 1992; 279:2
711) Deyo RA, Yezierski RP. “Descriptive epidemiology of low-back pain and its related medical care in the United States.” Spine 1987 ;12:264-8
712) van Tulder MW, et al. “A cost-of-illness study of back pain in the Netherlands.” Pain 1995 ;62:233-40
904) Freemont AJ, et al. “nerve in-growth into the diseased intervertebral disc in chronic back pain. Lancet, 1997 ;350:178-81
905) Palmgren T, et al. “ Imminohistochemical demonstration of sensory and autonomic nerve terminals in herniated lumbar disc tissue.” Spine 1996; 21:1301-1306
906) Coppes MH, et al. “Innervation of ‘painful’ lumbar discs.” Spine 1997; 22:2342-2349