Epidural Steroid Injections
Epidural Steroid Injections For Disc-Related Low Back Pain
 Although epidural steroid injections (ESIs) are typically thought of as a treatment for the radicular pain (leg pain), there is significant medical evidence that suggests ESIs can also be used to reduce the low-back pain associated with disc herniation and annular tear. [1-6]
Although epidural steroid injections (ESIs) are typically thought of as a treatment for the radicular pain (leg pain), there is significant medical evidence that suggests ESIs can also be used to reduce the low-back pain associated with disc herniation and annular tear. [1-6]
What is an epidural steroid injection? In a nutshell, an ESI, which have been around since the 1950s, is an outpatient medical procedure that involves inserting a thin needle into the epidural space at the level of the disc herniation or annular tear and then injecting 1.5-10mL a corticosteroid (a very powerful anti-inflammatory) and anesthetic into the area. The steroid will bathe the inflamed tissue in hopes of reducing that inflammation, thereby reducing the amount of patient-pain.
Who should perform the ESI procedure? Although many doctors of many different specialties are doing these procedures in this day and age of post-Obama care, only a fellowship-trained interventional pain medicine physician—one who has devoted his entire practice to using these injective procedures—would be good enough to treat my patients or me. [3]
Do epidural steroids really work? There has been a lot of quality research performed on epidural steroid injections, and the short answer is yes, they do work at least in the short term (< 6months) for the relief of back and leg pain associated with disc herniation. [2,7] However, if you have spondylolisthesis or have waited longer than a year to try them, then the chances of success are not as good. [7] It is, however, important to understand that there is no published medical research that demonstrates ESIs will have any effect on long-term clinical outcomes. [2] In other words, they are probably not going to affect how you are doing five years after the herniation or and or care occurs.
Epidural Steroid Injection: Fluoroscopic Guidance
Another very important component of the ESI procedure is fluoroscopic imaging, which should always be used in order to ensure correct needle placement.
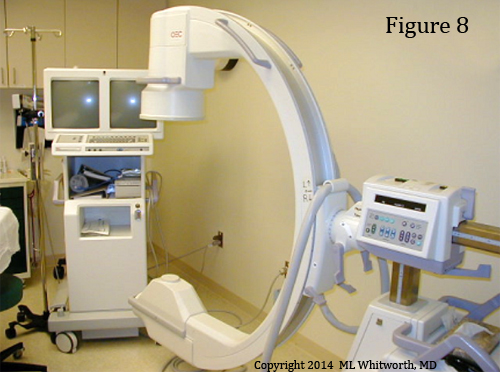
Specifically, the fluoroscopy machine (figure 8) uses a special low-level radiation to create a continuous radiographic picture (like the one created when you pass through security screening at the airport) of the low back.
During the ESI procedure, the physician will watch the monitors of the fluoroscopy machine in order to see exactly where the tip of the razor-sharp needle is, for even with fluoroscopy, it's not easy to place the needle precisely within the epidural space.
By using fluoroscopic guidance, not only is there an increased chance of properly placing the injectate (steroid + anesthetic), [8] but the chances of injuring the patient (intravenous injection, dural puncture, spinal cord contusion, nerve root injury) are greatly reduced. [9] Fluoroscopic guidance should always be used for ESI procedures, no matter which of the three approaches is used. [7]
Although using fluoroscopy during the procedure may sound like a no-brainer, you would be shocked at the number of physicians who don't use it. Despite what the physician may say to justify not using fluoroscopy, they are doing you a disservice by not using the, for medical research has demonstrated that these "blinded" ESI procedures (i.e., performed without the use of fluoroscopy) fail to get the injectate into the epidural space ( i.e., the target) 30-40% of the time! [7,8] Furthermore, by not using fluoroscopic guidance (or CT guidance) the risk of minor and major procedural complications significantly rises. [9] Therefore, I would not allow any of my patients or myself to undergo ESI without fluoroscopic guidance.
Frequency of Epidural Steroid Injections
The other thing to understand about ESIs is that the effect of the first injection may wear off fairly rapidly, so the entire procedure must be repeated within a few months. In fact, typically a patient who has responded to the first injection will need two more during the next 12 months. [3] However, if the first ESI fails to reduce your pain, then a second ESI will probably fail as well, and really shouldn't be attempted. [10]
Epidural Steroid Injections: Three Different Approaches
Caudal ESIs are performed by routing the needle through the narrow caudal canal of the sacrum and then releasing the steroid into the posterior epidural space (which of course is behind the thecal sac) only at the level of L5/S1. After its release the injectate must diffuse from the posterior epidural space, around the thecal sac, and (hopefully) enter the anterior epidural space in order to find its target (the disc herniation, annular tear, inflamed nerve root). Although this technique is still useful for patients who have suffered a lot of scar tissue (perineural fibrosis) in the anterior epidural space from a previous spine surgery, it has anecdotally really fallen out of favor because of its limitations and therefore is not encouraged. [3,7]
Interlaminar ESIs, which are still commonly used today, involve putting the needle between the lamina of the affected motion segment and then through the ligamentum flavum, which results in a "pop" and "loss of resistance" that the injectionist (doctor doing the procedure) can hear and feel. Like the caudal ESI, the injectate is released into the posterior epidural space and has to migrate around the thecal sac to the anterior epidural space in order to find its target. Again, some authors believe it "improbable" that the steroid will actually reach its target in the anterior epidural space and discourage the use of this procedure. [7]
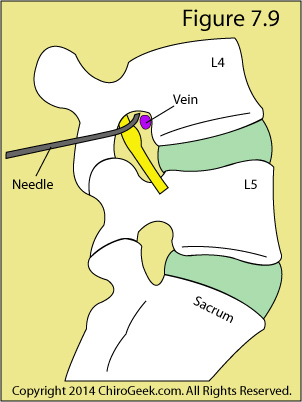
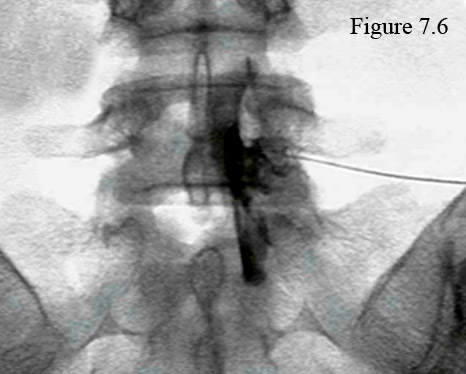
Transforaminal ESIs, which are very popular these days, involve placing the needle within the neural foramen of the affected motion segment, after which the steroid is released into the foramen and lateral anterior epidural space. The injectate now must travel only a short distance in order to reach the target. (figure 7.6 & 7.9)
Figure 7.9 is a para-sagittal cartoon through the neural foramina that demonstrates the traditional needle placement for a transforaminal ESI.
Note the good-sized vein that is in close proximity to the needle tip. Now, perhaps you may realize why using fluoroscopic guidance is so important when performing ESIs. Even with the use of fluoroscopy, there is vascular penetration of the needle tip into the vein 7.4% of the time. [9] Luckily, because of the fluoroscopic guidance, the injectionist will soon realize that he has "poked" the vein and will reposition the needle accordingly.
Too Much Steroid
Because of the long distance between the site of injection and the target, both interlaminar and caudal ESIs must use a significantly higher volume of steroid (typically ~9mL) in order to be effective. [4,6] Such a high volume of steroid can increase the risk for large spikes in blood glucose and blood pressure, which might not bode well for patients who are diabetic and/or hypertensive. On the other hand, because they are performed within the anterior epidural space, transforaminal ESIs use a much lower volume of steroid (typically ~3mL) yet are just as effective, if not more effective then the posterior epidural procedures. [5]
Personally, I have had both the interlaminar and transforaminal injections and, although they both eliminated back and leg pain, the transforaminal effect lasted much longer (one month) than the interlaminar injection (one week).
References
1) Parr AT, Diwan S, Abdi S. Lumbar interlaminar epidural injections in managing chronic low back pain and lower extremity pain: a systematic review. Pain Physician 2009;12:163-188.
2) Chou R, Atlas SJ, Stanos SP, Rosenquist RW. Nonsurgical interventional therapies for low back pain: a review of the evidence for an American Pain Society clinical practice guideline. Spine 2009;34:1078-1093.
3) Fetzer A, Scott DR. Nonsurgical treatment of herniated nucleus pulposus. In: Phillips FM, Lauryssen C, eds. The lumbar intervertebral disc. New York, NY: Thieme; 2010:86-91.
4) Manchikanti L, Cash KA, McManus CD, et al. A randomized, double-blind, active-controlled trial of fluoroscopic lumbar interlaminar epidural steroid injections in chronic axial or discogenic low back pain: results of two-year follow-up. Pain Physician to 13;16:E491-E504.
5) Rados I, Sakic K, Fingler M, et al. Efficacy of interlaminar versus transforaminal epidural steroid injection for the treatment of chronic unilateral radicular pain: prospective randomized study. Pain Medicine 2011; 12:1316-1321.
6) Parr AT, et al. Caudal epidural injections in the management of chronic low back pain: a systematic appraisal of the literature. Pain Physician 2012;15:E159-198.
7) Vad VB, Bhat AL, Lutz GE, et al. Transforaminal epidural steroid injections in lumbosacral radiculopathy: a prospective randomized study. Spine 2002; 27:11-16.
8) Weinstein SM, Herring SA, Derby R. Contemporary concepts in spine care: epidural steroid injections. Spine 1995; 20:184-186.
9) Karaman H, Kavak GO, Tufek A, et al. The complications of transforaminal lumbar epidural steroid injections. Spine 2011; 36:E819-E824.
10) Arden NK, et al. A multicenter randomized control trial of epidural corticosteroid injections for sciatica. Rheumatology 2005; 44:1399-1406.